Tobacco consumption patterns among iranian adults: a national and sub-national update from the steps survey 2021
- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
ABSTRACT Smoking is recognised as a critical public health priority due to its enormous health and economic consequences. Constant monitoring of the effectiveness of tobacco control programs
calls for timely population-based data. This study reports the national and sub-national patterns in tobacco consumption among Iranian adults based on the results from the STEPwise approach
to chronic disease risk factor surveillance (STEPS) survey 2021. This study was performed through an analysis of the results of the STEPS survey 2021 which had been conducted as a
nationally representative cross-sectional study. Participants included Iranian adults aged ≥ 18 years in all provinces of Iran, who were selected via multistage cluster sampling method. Data
were analyzed via survey analysis while considering population weights. The total number of participants was 27,874, including 15,395 (55.23%) women and 12,479 (44.77%) men. The all-ages
prevalence of current tobacco smoking was 14.01% overall, 4.44% among women, and 25.88% among men. The all-ages prevalence of current cigarette smoking was 9.33% overall, 0.77% among women,
and 19.95% among men. The all-ages prevalence of current hookah smoking was 4.5% overall, 3.64% among women, and 5.56% among men. The mean (SD) number of cigarettes smoked per day was 12.41
(10.27) overall, 7.65 (8.09) among women, and 12.64 (10.31) among men. The mean (SD) monthly times of hookah use was 0.42 (7.87) overall, 2.86 (23.46) among women, and 0.3 (6.2) among men.
The national all-ages prevalence of second-hand smoking at home was 24.64% overall, 27.38% among women, and 20.26% among men. The national all-ages prevalence of second-hand smoking at work
was 19.49% overall, 17.33% among women, and 22.94% among men. The tobacco consumption in Iran remains alarmingly high, indicating the current tobacco control policy implementation level is
ineffective and insufficient. This calls for adopting, implementing, and enforcing comprehensive packages of evidence-based tobacco control policies. SIMILAR CONTENT BEING VIEWED BY OTHERS
AGE OF TOBACCO SMOKING INITIATION AMONG IRANIAN ADULTS BASED ON NATIONAL AND SUBNATIONAL DATA FROM THE 2021 STEPS SURVEY Article Open access 12 March 2025 TRENDS IN CONCURRENT TOBACCO USE
AND HEAVY DRINKING AMONG INDIVIDUALS 15 YEARS AND OLDER IN MONGOLIA Article Open access 05 October 2022 PREDICTORS AND HEALTH OUTCOMES OF CIGARETTE AND SHISHA SMOKING AMONG MEN IN GAZA: A
CROSS-SECTIONAL STUDY Article Open access 23 August 2024 INTRODUCTION Smoking, the second leading risk factor for deaths and disability-adjusted life-years (DALYs), has caused more than 200
million deaths over the last three decades1. It has been recognised as a critical public health priority due to its enormous health and economic consequences2. As a modifiable risk factor,
the burden attributable to smoking could be minimised via the effective implementation of tobacco control interventions. Since the introduction of the World Health Organization (WHO)
Framework Convention on Tobacco Control (FCTC)3, countries have made endeavors to implement demand-reduction tools, including reducing affordability through taxation, passing smoke-free
laws, mandating health warnings on packaging, and banning tobacco advertising, promotion, and sponsorship4. Nevertheless, implementation and progress in tobacco control programs have varied
substantially across countries5. As the success of tobacco control programs has slowed in many countries in the past decade, it is estimated that the total number of smokers continues to
increase globally1. In this sense, constant monitoring of the effectiveness of previous tobacco control programs calls for timely population-based data on the prevalence of tobacco use for
taking prompt public health measures6. The STEPwise approach to chronic disease risk factor surveillance (STEPS), developed by WHO, focuses on obtaining data on established risk factors that
determine the burden of significant non-communicable diseases. The STEPS study has been conducted seven times in Iran in 2004, 2007, 2008, 2009, 2011, 2016 and 2021. This study reports the
national and sub-national smoking prevalence and tobacco consumption among Iranian adults based on the results from the STEPS survey 2021. METHODS ETHICS APPROVAL The study methodology
conformed to Helsinki Declaration standards as revised in 1989. All experimental protocols were approved by the National Institute for Health Research under reference number
IR.TUMS.NIHR.REC.1398.006. All participants provided written informed consent prior to participation in the study. Moreover, the data used in the study did not include any identifiable
personal information of participants, and the confidentiality of the data and the results are preserved. DATA SOURCE Data were derived from the STEPS study 2021, a national cross-sectional
survey carried out by the Non-Communicable Diseases Research Center (NCDRC). The STEPS survey required a nationally-representative sample. Five components were considered when estimating the
sample size, including the confidence interval, margin of error, design effect, baseline index level, and non-response rate. The sample size for evaluating risk factors of NCDs in each
province was calculated using a proportion to population size method. The survey used a systematic cluster classification method with 3176 clusters, each with ten participants, to conduct
the study on the national level. Iranian adults aged above 18 residing in urban or rural areas of one of the 31 provinces were studied as the target population, excluding certain individuals
such as those with mental disorders and pregnant women. In total, 28,821 participants from 3176 clusters were selected from rural and urban areas of the 31 provinces of Iran. A detailed
description of the study population and the sampling method of the 2021 version of the STEPS survey has been published elsewhere7. VARIABLES Smoking was assessed using the
transcultural-adaption of the STEPS questionnaire, as proposed by the World Health Organization (WHO) in national STEPS surveys. Covariates included sociodemographic status of participants
and their underlying conditions. Outcome variables included smoking-related variables. Sociodemographic variables included age, sex, province of residence, residential area, years of
schooling, marital status, employment status, health insurance, complementary insurance, and wealth. Underlying conditions included body mass index (BMI), hypertension, diabetes, and
cardiovascular diseases. Smoking-related variables included forms of smoking including cigarette smoking, hookah use, pipe smoking, and smokeless tobacco use; amount of cigarette smoking;
frequency of smoking; tobacco consumption; history of ex-smoking; attempt to quit smoking; history of second-hand smoking; and place of second-hand smoking. Current tobacco smoking was
defined as the use of smoked tobacco products, including cigarettes, pipes, or hookah, daily, non-daily or occasional basis in the past 12 months. Second-hand smoking, or passive smoking,
was defined as being exposed to the smoke of any tobacco products in the past 30 days. STATISTICAL ANALYSIS DATA WEIGHTING Data weighting was an important step between data cleaning and
analysis in this survey. It was necessary to deal with incomplete data and non-response, as well as differences in the population characteristics. To ensure the reliability and validity of
the results, a weighting procedure was used to adjust the survey data based on several factors. The four stages of the weighting procedure included: (a) weighting for general non-response,
(b) weighting for non-response at each step of the survey, (c) weighting for age, sex, and area of residence, and (d) final weighting for the analysis of data. More information on the
weighting process and equations used has been published elsewhere7. DESCRIPTIVE MEASURES Frequencies, proportions, means, and standard deviations were used to describe the data. We used the
chi-square test for categorised variables. T-test and one-way analysis of variance (ANOVA) test were used to analyse the differences among means of two groups and three groups or more,
respectively. We considered p-values below 0.05 as significant. AGE STANDARDISATION The National Population and Housing Census conducted by Iran's Statistical Center in 2016 was
considered the standard population for direct age-standardisation to allow comparisons between provinces8. INEQUITY ANALYSIS Principal Component Analysis (PCA) was applied to derive the
household wealth index based on questions on key dwelling characteristics and household ownership, as described in the study protocol. PCA is an approach to statistical analysis in which
multiple datasets are combined as orthogonal components9. The wealth index was used to divide the population into quintiles, whereby the first and fifth quintiles present the least fortunate
and wealthiest households, respectively. The concentration index with Erreygers' correction10 was used to quantify the degree of inequality in all types of smoking-related to wealth
index and years of schooling. A zero concentration index would indicate no inequality related to wealth index or years of schooling. Negative values of concentration index would mean a
higher prevalence of smoking among people with lower wealth index or years of schooling. Positive values of concentration index would indicate a higher prevalence of the type of smoking
among people with higher wealth index or years of schooling11. Model-based clustering method was applied to the data to achieve homogenous clusters regarding tobacco use on the sub-national
level based on the smoking behaviours reported. We used data mining methods to determine the number of clusters and the combination of provinces in each cluster12,13. TOOLS All essential
data analyses were performed using R statistical package v3.4.3 (http://www.r-project.org, RRID: SCR_001905). Data visualisations were performed using Python programming language, version
3.6 and R statistical package v3.4.3. RESULTS SOCIODEMOGRAPHIC STATUS The total number of participants was 27,874, including 15,395 (55.23%) women and 12,479 (44.77%) men. The
sociodemographic status of participants is presented in Table 1. PREVALENCE OF TOBACCO USE PREVALENCE OF TOBACCO USE AMONG WOMEN AND MEN OF ALL AGES The all-ages prevalence (95% CI) of
current tobacco smoking was 4.44% (4.09–4.82) among women, 25.88% (25.03–26.75) among men, and 14.01% (13.56–14.48) overall. The all-ages prevalence of current cigarette smoking was 0.77%
(0.62–0.95) among women, 19.95% (19.17–20.75) among men, and 9.33% (8.95–9.72) overall. The all-ages prevalence of current hookah smoking was 3.64% (3.33, 3.98) among women, 5.56%
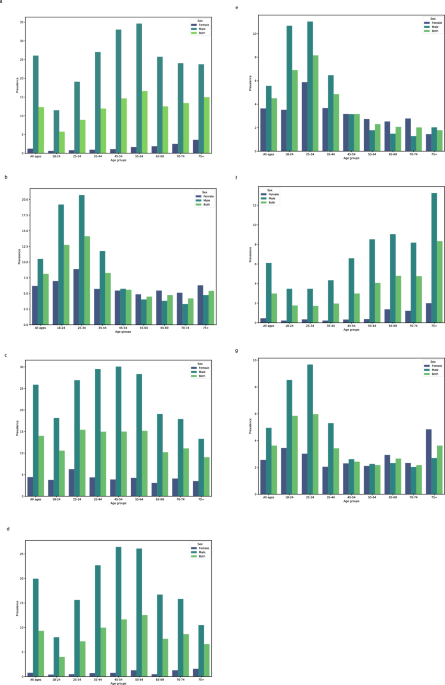
(5.12–6.03) among men, and 4.5% (4.23–4.78) overall. The all-ages prevalence of all types of tobacco smoking among both sexes is presented in Table 2. AGE PATTERN OF TOBACCO USE PREVALENCE
The prevalence (95% CI) of current cigarette smoking among men increased with age, from 8.01% (6.45–9.91) among men aged 18–24 to the observed peak of 26.43% (24.47–28.48) among age-group
45–54 years; however, it then decreased to 10.49% (8.08–13.51) among those aged more than 75. The prevalence of current use of hookah reached the observed peak of 11.03% (9.66, 12.56) among
men and 5.87% (4.98, 6.9) women aged 25–34, then decreased to 2.03% (1.1–3.72) among men aged more than 75 and 2.53% (1.66–3.85) among women aged 65–69. Some 19.19% (16.83–21.78) and 6.97%
(5.63–8.62) of men and women aged 18–24 years had used hookah at least once. The corresponding rates were 20.7% (18.91–22.61) and 8.88% (7.77–10.13) for men and women aged 25–34 years,
respectively (Fig. 1, Supplementary Table 1). GEOGRAPHICAL PATTERN OF TOBACCO PREVALENCE The age-standardised (95% CI) prevalence of all types of smoking varied significantly across the 31
provinces of Iran (Fig. 2a–c, Supplementary Table 2). GEOGRAPHICAL PATTERN OF TOBACCO PREVALENCE AMONG WOMEN The age-standardised prevalence (95% CI) of ever smoking among women ranged from
0.81% (0.19–3.35) in Ilam to 20.87% (17.62–24.54) in Sistan and Baluchistan. The prevalence of ever cigarette smoking among women ranged from Zero percent in Ilam, Hormozgan, Sistan and
Baluchistan, and South Khorasan to 2.19% (1.19–4) in West Azerbaijan. The prevalence of ever use of hookah among women ranged from 0.23% (0.03–1.59) in Ardabil to 19.5% (16.38–23.06) in
Sistan and Baluchistan. The prevalence of current smoking among women ranged from 0.39% (0.12–1.29) in Chahar Mahaal and Bakhtiari to 16.64% (13.69–20.08) in Sistan and Baluchistan. The
prevalence of current cigarette smoking among women ranged from zero percent in Bushehr, Chahar Mahaal and Bakhtiari, Hormozgan, Ilam, North Khorasan Sistan, South Khorasan, Markazi, and
Baluchistan to 1.59% (1.04–2.43) in Tehran. The prevalence of the current use of hookah among women ranged from zero percent in Ardabil and West Azerbaijan to 15.27% (12.47–18.56) in Sistan
and Baluchistan (Fig. 2b, Supplementary Table 2). GEOGRAPHICAL PATTERN OF TOBACCO PREVALENCE AMONG MEN The age-standardised prevalence (95% CI) of ever smoking among men ranged from 20.94%
(16.19–26.65) in South Khorasan to 45.99% (39.71–52.39) in Qazvin. The prevalence of ever cigarette smoking among men ranged from 13.28% (9.65–18.01) in South Khorasan to 39.02%
(33.05–45.34) in Qazvin. The prevalence of ever use of hookah among men ranged from 3.68% (1.96–6.81) in Kermanshah to 22.38% (12.63–20.63) in Isfahan. The prevalence of current smoking
among men ranged from 12.88% (9.31–17.57) in South Khorasan to 38.21% (32.25–44.55) in Qazvin. The prevalence of current cigarette smoking among men ranged from 7.29% (4.77–10.97) in South
Khorasan to 32.39% (26.87–38.44) in Qazvin. The prevalence of current use of hookah among men ranged from 2.81% (1.38–5.66) in Kermanshah to 12.32% (9.31–16.12) in Isfahan (Fig. 2c,
Supplementary Table 2). CIGARETTE AND HOOKAH SMOKING CIGARETTE AND HOOKAH SMOKING AMONG WOMEN AND MEN The all-ages mean (SD) cigarette pack/year was 17.56 (19.32) overall, 11.93 (17.35)
among women, and 17.83 (19.37) among men. The mean (SD) number of cigarettes smoked per day was 12.41 (10.27) overall, 7.65 (8.09) among women, and 12.64 (10.31) among men. The mean (SD)
monthly times of hookah use was 0.42 (7.87) overall, 2.86 (23.46) among women, and 0.3 (6.2) among men (Fig. 3, Supplementary Table 3). AGE PATTERN OF CIGARETTE AND HOOKAH SMOKING The mean
(SD) number of cigarettes smoked per day increased with age, from 9 (9) among men and 4.28 (5.02) among women aged 18–24 to the observed peak of 13.87 (10.08) among men and 14.64 (7.73)
among women aged 65–69 (Fig. 3, Supplementary Table 3). GEOGRAPHICAL PATTERN OF CIGARETTE AND HOOKAH SMOKING Cigarette and hookah smoking varied significantly among men and women across the
31 provinces of Iran (Fig. 4a–c, and Supplementary Table 4). GEOGRAPHICAL PATTERN OF CIGARETTE AND HOOKAH SMOKING AMONG WOMEN Among provinces with enough data, the mean cigarette pack/year
ranged from 0.03 in Qazvin to 45 in Gilan. The median cigarette pack/year ranged from 0.03 in Qazvin to 45 in Gilan. The mean number of cigarettes smoked per day ranged from 0.03 in Qazvin
to 18. 61 in Hamadan. The median number of cigarettes smoked per day ranged from 0.03 in Qazvin to 20 in Kermanshah, Gilan, Lorestan, and Fars. The mean monthly times of hookah use ranged
from Zero in Alborz, Ardebil, East Azerbaijan, West Azerbaijan, Fars, Gilan, Golestan, Hamadan, Isfahan, Kerman, Kermanshah, Khuzestan, Lorestan, Mazandaran, Qazvin, Semnan, and Zanjan to
7.31 in Terhan. The median monthly times of hookah use ranged from Zero in Alborz, Ardebil, East Azerbaijan, West Azerbaijan, Fars, Gilan, Golestan, Hamadan, Isfahan, Kerman, Kermanshah,
Razavi Khorasan, Khuzestan, Kurdistan, Kohgiluyeh and Boyer − Ahmad, Lorestan, Mazandaran, Qazvin, Semnan, Tehran and Zanjan to 4.29 in Qom and Yazd (Fig. 4b, Supplementary Table 4).
GEOGRAPHICAL PATTERN OF CIGARETTE AND HOOKAH SMOKING AMONG MEN The mean cigarette pack/year ranged from 10.28 in Sistan and Baluchistan to 24.9 in West Azerbaijan. The median cigarette
pack/year ranged from 4.5 in Kerman to 19.2 in Qom. The mean number of cigarettes smoked per day ranged from 7.93 in Razavi Khorasan to 17.4 in West Azerbaijan. The median number of
cigarettes smoked per day ranged from 6 in Razavi Khorasan to 20 in West Azerbaijan and East Azerbaijan. The mean monthly times of hookah use ranged from zero in Ardebil, Chahar Mahaal and
Bakhtiari, Hormozgan, Ilam, North Khorasan, South Khorasan, and Qazvin to 5.24 in Sistan and Baluchistan. The median monthly times of hookah use was zero in all provinces (Fig. 4a,
Supplementary Table 4). PREVALENCE OF SECOND-HAND SMOKING PREVALENCE OF SECOND-HAND SMOKING AT HOME The national all-ages prevalence (95% CI) of second-hand smoking at home was 24.64
(24.05–25.24) overall, 27.38 (26.59–28.18) among women, and 20.26 (19.39–21.17) among men. The prevalence of second-hand smoking at home decreased with age among both sexes, from 29.35%
(27.39–31.39) among age-group 18–24 to 16.17% (13.74–18.93) among those aged 70–74. It then rose to 18.72% (16.22–21.52) among those aged more than 75. The prevalence of second-hand smoking
at home among women ranged from 14.94% (11.11–19.79) % in Alborz to 48.9% (43.5–54.33) in Kerman. The prevalence of second-hand smoking at home among men ranged from 8.2% (5–13.17) in Alborz
to 39.14% (32.84–45.83) in Kerman (Figs. 2, 5, Supplementary Tables 1, 2). PREVALENCE OF SECOND-HAND SMOKING AT WORK The national all-ages prevalence (95% CI) of second-hand smoking at work
was 19.49% (18.95–20.05) overall, 17.33% (16.67–18.02) among women, and 22.94% (22.01–23.9) among men. The prevalence of second-hand smoking at work among both sexes increased from 22.92%
(21.11–24.84) among age-group 18–24 to 23.98% (22.62–25.39) among age-group 25–34. The prevalence of second-hand smoking at work among women ranged from 6.91% (4.47–10.53) in Semnan to 36.7%
(31.91–41.77) in Kurdistan. The prevalence of second-hand smoking at work among men ranged from 14.37% (10.06–20.1) in South Khorasan to 43.44% (35.72–51.49) in Ardabil (Figs. 1, 5,
Supplementary Tables 1, 2). DETERMINANTS OF TOBACCO SMOKING WEALTH AND YEARS OF SCHOOLING On the national level, lower wealth index or years of schooling were associated with higher
prevalence of ever or current tobacco smoking among both women and men (Table 3). Nevertheless, wealth index and years of schooling had varying roles in tobacco smoking prevalence among
women and men across provinces in Iran (Fig. 6, Supplementary Table 5). GEOGRAPHICAL PATTERN Using model-based clustering, the 31 provinces of Iran were categorized into four clusters based
on prevalence of ever tobacco smoking, ever cigarette smoking, current tobacco smoking, and current cigarette smoking (Fig. 7). The prevalence of smoking among the four clusters is presented
in Table 4. DISCUSSION The study showed that 14% of the Iranian adults, 4.4% of women and 25.9% of men, were current tobacco smokers in 2021. Some 9.3% of the study participants, 0.8% of
women and 20% of men, were current cigarette smokers. Moreover, the all-ages prevalence of current hookah use was 3.6% among women and 5.6% among men. Pipe smoking and smokeless tobacco were
unpopular among the Iranian population. The prevalence of current tobacco smoking since the previous STEPS survey in 2016 has stagnated: form 14.1% in 2016 to 14% in 2021. Nevertheless, the
mean number of cigarettes smoked per day has increased from 10.4 in 2016 to 12.4 in 202114. There was a heterogeneous geographical distribution pattern in tobacco smoking prevalence in
Iran, distinctively witnessed among the smoking behaviour of women and men, depending on the type of smoking. In northwestern Iran, West Azerbaijan had the second-highest prevalence of
current cigarette smoking among men and the fourth-highest among women. Nevertheless, it ranked 16th in terms of current hookah use among men, and the prevalence was nearly zero among women.
In southwestern Iran, Bushehr had the highest prevalence of current hookah use among both women and men, while having nearly zero prevalence of current cigarette smoking among women and
being ranked as the third-lowest in terms of prevalence among men. In southeastern Iran, women in Sistan and Baluchistan had the second-highest prevalence of current hookah use while having
nearly zero prevalence of current cigarette smoking. Sistan and Baluchistan also had the highest prevalence of smokeless tobacco use. The geographical pattern also conformed to neighbouring
countries1,15, possibly due to ethnic, cultural, and access resemblance16. Using data mining techniques, we grouped Iran’s provinces into four clusters with similar prevalence of ever
tobacco smoking, ever cigarette smoking, current tobacco smoking, and current cigarette smoking. In provinces in cluster 1, smoking cessation policies need to be prioritized, while other
forms of tobacco use, namely hookah are less pressing issues. In cluster 2, which interestingly maps to northwestern Iran, both cigarette smoking and tobacco use need to be addressed. In
provinces in cluster 3 both ever/current prevalence of tobacco and cigarette smoking are low. Cluster 4 is consistent with central, southern, and eastern provinces, where tobacco consumption
needs to be addressed. The clustering of provinces could empower Iranian authorities in decision-making and public policy efforts regarding tobacco control. This needs to be further
investigated in future studies which particularly focus on proposing tobacco reduction policies based on the real-world data. Notably, upon interpretation of the results of model-based
clustering, the role of smoking determinants reported in this study including wealth index and years of schooling need to be considered for policy and intervention development. The
prevalence gap between men and women was narrower in the current hookah use compared with current cigarette smoking. The prevalence of hookah use is more than cigarette smoking among women.
Moreover, women tend to have more positive attitudes towards hookah use, which is much less stigmatised than cigarette smoking17. In recent years, the prevalence of hookah use among women
has increased more than men18. Alarmingly, the study showed that women's mean monthly times of hookah use was more than nine times that of men. Meanwhile, there is evidence that the
deleterious effects of hookah use on women could be higher than in men19. There was an interest in hookah use, particularly among younger adults. Some 19% and 7% of men and women aged 18–24
years had used hookah at least once. Moreover, the prevalence of current hookah use reached a surprisingly early peak of 11% among men and 6% women aged 25–34. Despite supposedly more
deleterious effects of hookah use than cigarette smoking20, there has been a growing interest in hookah use in recent decades21. While hookah use is considered recreational in Iran16, there
is evidence that hookah users are increasingly susceptible to cigarette smoking22,23. Six decades after the first documentations of the deleterious health effects of tobacco use24, there has
been substantial progress in reducing the prevalence of tobacco smoking worldwide. In contrast, it is estimated that the age-standardised prevalence of current tobacco smoking has increased
by 8% among men and 2% among women in the past three decades in Iran and the population growth has also led to a marked increase in the number of smokers1. Since introducing the WHO
Framework Convention on Tobacco Control (FCTC) in 2005, outlining demand-reduction policies, many counties have witnessed drastic decreases in the prevalence of tobacco smoking25. Taking a
closer look at the previous STEPS surveys in Iran, the smoking prevalence of Iranian adults has somewhat stagnated since 2004 among both men and women26. Simultaneously, Brazil, Norway, and
Senegal have managed to decrease the prevalence of tobacco smoking by 73%, 54%, and 51%, respectively. Iceland, Denmark, Canada, Australia, Colombia, and Costa Rica, also witnessed nearly
50% decreases in the prevalence of tobacco smoking1. Though once an early adapter to FCTC16, the current tobacco control policy implementation level is insufficient in Iran. In the absence
of any new concerted effort towards smoking reduction, sanctions and subsequently the economic downturn could have played a significant role in the slight reduction of smoking prevalence in
Iran since 201614,16,27. Evidence shows that economic recessions are associated with decreased cigarette consumption via decreasing its affordability16. Overall, cigarettes have become less
affordable in Iran, particularly since 201828. The purchase pattern of Iranian smokers has changed from the whole box of cigarettes to the single stick cigarette. In addition, smokers have
generally swapped to less expensive cigarettes29. Dealing with the burden attributable to tobacco use, public health authorities encounter substantial obstacles such as an increased number
of smokers due to population growth, pressure from the tobacco industry, and competing for health and political priorities1. WHO discourages Iran from implementing high import duties as they
encourage domestic production of tobacco. Direct taxation also needs to be excised rather than other indirect taxes. Moreover, uniform tax rates are recommended to avoid product
switching28. There is evidence that tobacco taxation, as one of the most cost-effective tobacco control policies30, needs to be concordantly adjusted to people's purchasing power to
remain potent and reduce affordability31. Moreover, the revenue from tobacco taxation needs to be redistributed to tobacco control programs, health care services, and social support
services30. Unless strict regulations are in place to control cigarette smuggling, any increase in cigarette price could be compensated by flooding smuggled cigarettes into the market29.
This calls for substantially reducing smoking rates in the country via adopting, implementing, and enforcing comprehensive packages of evidence-based tobacco control policies. The witnessed
heterogeneities and determinants in the patterns of smoking prevalence and tobacco consumption need to be taken into account when prioritizing vulnerable groups and designing tobacco
reduction strategies, especially considering the relative authority of the medical universities of Iran in sub-national healthcare programs implementation32. Otherwise, the death toll,
imposed economic costs, and the burden to health systems caused by smoking will increase over the years. STRENGTHS AND LIMITATIONS The main strength of this study lies in its large sample
size. Given the sampling method, the results could represent the Iranian population. The study investigated the smoking prevalence and tobacco consumption pattern by age, sex, province of
residence, wealth, and years of schooling. This could empower public health authorities to make evidence-based decisions and design tobacco reduction action plans based on various
determinants according to real-world data, especially considering that individual level data were used for assessing the inequality patterns. Moreover, this was the first nationwide study
from Iran to investigate pipe smoking and the use of smokeless tobacco. Given the use of electronic and online data gathering tools, the study had very little missing data. To minimise the
missing data, the software used for data collection was designed to avoid ignoring obligatory questions. Moreover, the estimated sample size was initially calculated to be 10% higher than
the required sample size so that potential missing data did not violate the sample representativeness. CONCLUSION The tobacco consumption in Iran remains alarmingly high, indicating the
current tobacco control policy implementation level is insufficient. This calls for adopting, implementing, and enforcing comprehensive packages of evidence-based tobacco control policies.
In the meantime, the witnessed heterogeneities in the patterns of smoking prevalence and tobacco consumption need to be considered when designing tobacco reduction strategies. Otherwise, the
death toll, imposed economic costs, and the burden to health systems caused by smoking will increase over the years. DATA AVAILABILITY The datasets used and analysed during the current
study available from the corresponding author on reasonable request. REFERENCES * Reitsma, M. B. _et al._ Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and
attributable disease burden in 204 countries and territories, 1990–2019: A systematic analysis from the Global Burden of Disease Study 2019. _Lancet_ 397, 2337–2360 (2021). Article Google
Scholar * Jha, P. & Peto, R. Global effects of smoking, of quitting, and of taxing tobacco. _N. Engl. J. Med._ 370, 60–68 (2014). Article CAS PubMed Google Scholar * W. H.
Organization. _WHO Framework Convention on Tobacco Control_. (2003). * Chung-Hall, J., Craig, L., Gravely, S., Sansone, N. & Fong, G. T. Impact of the WHO FCTC over the first decade: A
global evidence review prepared for the Impact Assessment Expert Group. _Tob. Control_ 28, S119–S128 (2019). Article PubMed Google Scholar * World Health Organization. _WHO Report on the
Global Tobacco Epidemic, 2019 : Offer Help to Quit Tobacco Use_ (2019). * Bilano, V. _et al._ Global trends and projections for tobacco use, 1990–2025: An analysis of smoking indicators from
the WHO comprehensive information systems for tobacco control. _Lancet_ 385, 966–976 (2015). Article PubMed Google Scholar * _Protocol Design for Surveillance of Risk Factors of
Non-Communicable Diseases During the COVID-19 Pandemic: An Experience from Iran STEPS Survey 2021_. http://journalaim.com/Article/aim-23947 (2021). * Statistical Center of Iran. _Population
and Housing Censuses_. https://www.amar.org.ir/english/Population-and-Housing-Censuses. * Rencher, A. C. & Schimek, M. G. Methods of multivariate analysis. _Comput. Stat._ 12, 422
(1997). Google Scholar * Erreygers, G. Correcting the concentration index. _J. Health Econ._ 28, 504–515 (2009). Article PubMed Google Scholar * O’Donnell, O., O’Neill, S., Van Ourti, T.
& Walsh, B. conindex: Estimation of concentration indices. _Stand. Genomic Sci._ 16, 112 (2016). Google Scholar * Parsaeian, M. _et al._ Introducing an efficient sampling method for
national surveys with limited sample sizes: Application to a national study to determine quality and cost of healthcare. _BMC Public Health_ 21, 1–10 (2021). Article Google Scholar *
Abbasi-Kangevari, M. _et al._ Quality and cost of healthcare services in patients with diabetes in Iran: Results of a nationwide short-term longitudinal survey. _Front. Endocrinol._ 14,
1099464 (2023). Article Google Scholar * Varmaghani, M. _et al._ Prevalence of smoking among Iranian adults: Findings of the national steps survey 2016. _Arch. Iran. Med._ 23, 369–377
(2020). Article PubMed Google Scholar * Kendrick, P. J. _et al._ Spatial, temporal, and demographic patterns in prevalence of chewing tobacco use in 204 countries and territories,
1990–2019: A systematic analysis from the Global Burden of Disease Study 2019. _Lancet Public Health_ 6, e482–e499 (2021). Article Google Scholar * Sohrabi, M.-R., Abbasi-Kangevari, M.
& Kolahi, A.-A. Current tobacco smoking prevalence among Iranian population: A closer look at the STEPS surveys. _Front. Public Health_ 8, 571062 (2020). Article PubMed PubMed Central
Google Scholar * Burki, T. K. Tobacco control in Jordan. _Lancet Respir. Med._ 7, 386 (2019). Article PubMed Google Scholar * Dadipoor, S. _et al._ Explaining the determinants of
hookah consumption among women in southern Iran: A qualitative study. _BMC Public Health_ 19, 1–13 (2019). Article Google Scholar * Salameh, P., Khayat, G. & Waked, M. Lower prevalence
of cigarette and waterpipe smoking, but a higher risk of waterpipe dependence in Lebanese adult women than in men. _Women Health_ 52, 135–150 (2012). Article PubMed Google Scholar *
Jukema, J. B., Bagnasco, D. E. & Jukema, R. A. Waterpipe smoking: not necessarily less hazardous than cigarette smoking: Possible consequences for (cardiovascular) disease. _Neth. Hear.
J._ 22, 91 (2014). Article CAS Google Scholar * Qasim, H. _et al._ The effects of hookah/waterpipe smoking on general health and the cardiovascular system. _Environ. Health Prevent. Med._
24, 1–17 (2019). Article Google Scholar * Bahelah, R. Curiosity and susceptibility to cigarette smoking among cigarette-naïve, waterpipe smoking US youth: National Youth Tobacco Survey,
2014. _Tobacco Prevent. Cessation_ 3, 132 (2017). Google Scholar * Soneji, S., Sargent, J. D., Tanski, S. E. & Primack, B. A. Associations between initial water pipe tobacco smoking and
snus use and subsequent cigarette smoking: Results from a longitudinal study of US adolescents and young adults. _JAMA Pediatr._ 169, 129–136 (2015). Article PubMed PubMed Central Google
Scholar * Doyle, J. T., Dawber, T. R., Kannel, W. B., Heslin, A. S. & Kahn, H. A. Cigarette smoking and coronary. _Heart Dis._ https://doi.org/10.1056/NEJM196204192661602266,796-801
(2009). Article Google Scholar * Gravely, S. _et al._ Implementation of key demand-reduction measures of the WHO Framework Convention on Tobacco Control and change in smoking prevalence in
126 countries: An association study. _Lancet Public Health_ 2, e166–e174 (2017). Article PubMed Google Scholar * Sohrabi, M.-R., Abbasi-Kangevari, M. & Kolahi, A.-A. Current tobacco
smoking prevalence among Iranian population: A closer look at the STEPS surveys. _Front. Public Health_ 8, 945 (2020). Article Google Scholar * Abbasi-Kangavari, M. _et al._ Current
inequities in smoking prevalence on district level in Iran: A systematic analysis on the STEPS survey. _J. Res. Health Sci._ 22, e00540 (2021). Article PubMed Google Scholar *
Mediterranean, W. H. Organization. _R. O. for the E. Tobacco Tax: Islamic Republic of Iran_. * Golestan, Y. P. _et al._ The effect of price on cigarette consumption, distribution, and sale
in Tehran: A qualitative study. _BMC Public Health_ 21, 1–9 (2021). Article Google Scholar * WHO. _Earmarked Tobacco Taxes: Lessons Learnt from Nine Countries_. _Preprint_ (2016). *
Institute, U. N. C. & WHO. _Monograph 21. The Economics of Tobacco and Tobacco Control. Preprint_ (2016). * Peykari, N. _et al._ National action plan for non-communicable diseases
prevention and control in Iran; A response to emerging epidemic. _J. Diabetes Metab. Disord._ 16, 3 (2017). Article PubMed PubMed Central Google Scholar Download references AUTHOR
INFORMATION Author notes * These authors contributed equally: Mohsen Abbasi-Kangevari, Ali Ghanbari and Nima Fattahi. AUTHORS AND AFFILIATIONS * Non-Communicable Diseases Research Center,
Endocrinology and Metabolism Population Sciences Institute, Tehran University of Medical Sciences, Tehran, Iran Mohsen Abbasi-Kangevari, Ali Ghanbari, Nima Fattahi, Mohammad-Reza Malekpour,
Masoud Masinaei, Naser Ahmadi, Seyyed-Hadi Ghamari, Mohammadreza Naderian, Mohammad-Mahdi Rashidi, Negar Rezaei, Erfan Ghasemi, Yosef Farzi, Moein Yoosefi, Nazila Rezaei, Elmira Foroutan
Mehr, Mana Moghimi, Maryam Nasserinejad, Ali Maleki, Zeinab Abbasi-Kangevari & Farshad Farzadfar * Department of Internal Medicine, Yale School of Medicine, New Haven, CT, USA Nima
Fattahi * Department of Epidemiology and Biostatistics, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran Masoud Masinaei * Tehran Heart Center, Cardiovascular
Diseases Research Institute, Tehran University of Medical Sciences, Tehran, Iran Mohammadreza Naderian * Endocrinology and Metabolism Research Center, Endocrinology and Metabolism Clinical
Sciences Institute, Tehran University of Medical Sciences, Tehran, Iran Negar Rezaei & Farshad Farzadfar Authors * Mohsen Abbasi-Kangevari View author publications You can also search
for this author inPubMed Google Scholar * Ali Ghanbari View author publications You can also search for this author inPubMed Google Scholar * Nima Fattahi View author publications You can
also search for this author inPubMed Google Scholar * Mohammad-Reza Malekpour View author publications You can also search for this author inPubMed Google Scholar * Masoud Masinaei View
author publications You can also search for this author inPubMed Google Scholar * Naser Ahmadi View author publications You can also search for this author inPubMed Google Scholar *
Seyyed-Hadi Ghamari View author publications You can also search for this author inPubMed Google Scholar * Mohammadreza Naderian View author publications You can also search for this author
inPubMed Google Scholar * Mohammad-Mahdi Rashidi View author publications You can also search for this author inPubMed Google Scholar * Negar Rezaei View author publications You can also
search for this author inPubMed Google Scholar * Erfan Ghasemi View author publications You can also search for this author inPubMed Google Scholar * Yosef Farzi View author publications You
can also search for this author inPubMed Google Scholar * Moein Yoosefi View author publications You can also search for this author inPubMed Google Scholar * Nazila Rezaei View author
publications You can also search for this author inPubMed Google Scholar * Elmira Foroutan Mehr View author publications You can also search for this author inPubMed Google Scholar * Mana
Moghimi View author publications You can also search for this author inPubMed Google Scholar * Maryam Nasserinejad View author publications You can also search for this author inPubMed
Google Scholar * Ali Maleki View author publications You can also search for this author inPubMed Google Scholar * Zeinab Abbasi-Kangevari View author publications You can also search for
this author inPubMed Google Scholar * Farshad Farzadfar View author publications You can also search for this author inPubMed Google Scholar CONTRIBUTIONS Conceptualization: F.F., Ne.R.,
M.A.-K.; Data curation: F.F., Ne.R., Na.R., Y.F., E.G., M.Y., E.F.M., M.N., M-M.R., N.F., N.A., M.Ma., A.G.; Formal Analysis: A.G., M.Ma., N.A., M-R.M., E.G., M.N., M.A.-K.; Funding
acquisition: F.F.; Investigation: F.F., Ne.R.; Methodology: F.F., Ne.R., M.-R.M., N.A., M.Ma., A.G.; Project administration: F.F., Ne.R.; Resources: F.F., Ne.R., Na.R.; Supervision: F.F.,
Ne.R.; Validation: F.F., Ne.R., A.G., M.Ma., N.A., M-R.M., M.A.-K.; Visualisation: M.A.-K., M.-R.M., M.Ma.; Writing-original draft: M.A.-K.; Writing-review & editing: M.A.-K., A.G.,
M.-R.M., M.Ma., N.A., S.-H.G., M.N., N.F., M.-M.R., A.M., Z.A.-K., Na.R., E.F.M., M.Mo., Ne.R., F.F. CORRESPONDING AUTHOR Correspondence to Farshad Farzadfar. ETHICS DECLARATIONS COMPETING
INTERESTS The authors declare no competing interests. ADDITIONAL INFORMATION PUBLISHER'S NOTE Springer Nature remains neutral with regard to jurisdictional claims in published maps and
institutional affiliations. SUPPLEMENTARY INFORMATION SUPPLEMENTARY TABLE 1. SUPPLEMENTARY TABLE 2. SUPPLEMENTARY TABLE 3. SUPPLEMENTARY TABLE 4. SUPPLEMENTARY TABLE 5. RIGHTS AND
PERMISSIONS OPEN ACCESS This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any
medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The
images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is
not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission
directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE
Abbasi-Kangevari, M., Ghanbari, A., Fattahi, N. _et al._ Tobacco consumption patterns among Iranian adults: a national and sub-national update from the STEPS survey 2021. _Sci Rep_ 13, 10272
(2023). https://doi.org/10.1038/s41598-023-37299-3 Download citation * Received: 18 November 2022 * Accepted: 20 June 2023 * Published: 24 June 2023 * DOI:
https://doi.org/10.1038/s41598-023-37299-3 SHARE THIS ARTICLE Anyone you share the following link with will be able to read this content: Get shareable link Sorry, a shareable link is not
currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative