Eosinopenia and neutrophil-to-lymphocyte count ratio as prognostic factors in exacerbation of copd
- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
ABSTRACT Exacerbations of Chronic Obstructive Pulmonary Disease (AECOPDs) are one of the most important clinical aspects of the disease, and when requiring hospital admission, they
significantly contribute to mortality among COPD patients. Our aim was to assess the role of eosinopenia and neutrophil-to-lymphocyte count (NLR) as markers of in-hospital mortality and
length of hospitalization (LoH) among patients with ECOPD requiring hospitalization. We included 275 patients. Eosinopenia was associated with in-hospital deaths only when coexisted with
lymphocytopenia, with the specificity of 84.4% (95% CI 79.6–88.6%) and the sensitivity of 100% (95% CI 35.9–100%). Also, survivors presented longer LoH (P < 0.0001). NLR ≥ 13.2 predicted
in-hospital death with the sensitivity of 100% (95% CI 35.9–100%) and specificity of 92.6% (95% CI 88.8–95.4%), however, comparison of LoH among survivors did not reach statistical
significance (P = 0.05). Additionally, when we assessed the presence of coexistence of eosinopenia and lymphocytopenia first, and then apply NLR, sensitivity and specificity in prediction of
in-hospital death was 100% (95% CI 35.9–100) and 93.7% (95% CI 90.1–96.3), respectively. Moreover, among survivors, the occurrence of such pattern was associated with significantly longer
LoH: 11 (7–14) vs 7 (5–10) days (P = 0.01). The best profile of sensitivity and specificity in the prediction of in-hospital mortality in ECOPD can be obtained by combined analysis of
coexistence of eosinopenia and lymphocytopenia with elevated NLR. The occurrence of a such pattern is also associated with significantly longer LoH among survivors. SIMILAR CONTENT BEING
VIEWED BY OTHERS PROGNOSTIC VALUE OF THE PLATELET, NEUTROPHIL, MONOCYTE, BASOPHIL, AND EOSINOPHIL TO LYMPHOCYTE RATIOS IN PATIENTS WITH SEVERE COMMUNITY-ACQUIRED PNEUMONIA (SCAP) Article
Open access 06 December 2024 EFFECTS OF LYMPHOCYTE AND NEUTROPHIL COUNTS AND THEIR TIME COURSES ON MORTALITY IN PATIENTS WITH POSTOPERATIVE PNEUMONIA Article Open access 26 August 2022
PROGNOSTIC VALUE OF NEUTROPHIL-TO-LYMPHOCYTE RATIO IN COVID-19 COMPARED WITH INFLUENZA AND RESPIRATORY SYNCYTIAL VIRUS INFECTION Article Open access 02 November 2021 INTRODUCTION
Exacerbations of chronic obstructive pulmonary disease (AECOPDs) are one of the most important clinical aspects to the disease. The clinical manifestations of COPD exacerbations are highly
variable and reflect broad heterogeneity in the pathobiology of the disease. Regardless of its variability, exacerbations are clearly associated with negative impact on the health status,
increasing rates of hospitalization, readmission, and disease progression1,2,3. AECOPDs requiring hospital admission are the leading cause of hospitalization and significantly contribute to
mortality among COPD patients4. Therefore, research on prognostic factors in this group is of special interest. With a great deal of reasonable criticism, eosinopenia was already proposed as
a marker of infection, in differentiating infectious from non-infectious causes of elevated C-reactive protein (CRP) and identifying sepsis or bacteremia5. Eosinopenia was also proposed to
be a predictor of a short or long-term survival in some diseases, including AECOPD6,7,8,9,10. Thus, we reanalyzed the problem of eosinopenia in AECOPD patients. Additionally, we assessed
another previously discussed, and logically linked with eosinopenia, prognostic factor—neutrophil-to-lymphocyte count (NLR). This parameter has also been studied as a marker of sepsis and
predictor of bacteriemia5. The roles of both these parameters in AECOPD still remain ambiguous and controversial. The aim of this study was to assess the role of eosinopenia and NLR as
markers of in-hospital mortality and length of hospitalization. The relationships between both parameters and their possible pathophysiological background were analyzed as well. PATIENTS AND
METHODS This study is a retrospective analysis of the data collected in the digital base of the Barlicki Memorial Teaching Hospital of the Medical University of Lodz. The protocol of the
study was approved by the institutional ethics committee. Also, due to retrospective character of the study, in which consent would be impossible to obtain, concordantly with the Declaration
of Helsinki, the Committee waived the need of such consent. All methods in the study were performed in accordance with the relevant guidelines and regulations. Enrollment of our study
included only adult Caucasians with the exacerbation of COPD, diagnosed concordantly with current GOLD recommendations3. We included only exacerbations that required hospital admission, both
of infectious and non-infectious character. Full blood count and white blood cell differentiation were examined in these patients, which was performed on the hospital admission. Venous
blood was collected by venipuncture into tubes with ethylenediaminetetraacetic acid as an anticoagulant. The samples were examined with the automated hematology analyzer. Cell counting was
performed using electrical impedance method. Arterial blood gases parameters were analyzed using automated analyzer. The exclusion criteria were any other known chronic lung disease, any
hematological disorder—active, or in the past medical history, any active malignancy, exacerbation of respiratory symptoms associated with other acute causes. We also excluded patients with
clinically and radiologically proven pneumonia and those, who received any dose of systemic corticosteroids prior to the admission. Additionally, we excluded all patients who were
transferred to the hospital by an ambulance, because retrospective character of the study would preclude reliable verification that these patients did not receive corticosteroids prior to
the hospital admission. AECOPD was defined as an event characterized by a rapid decline in the patient’s respiratory symptoms that is beyond normal day-to-day variations and lead to changes
in medication. In-hospital mortality was defined as any AECOPD-related death after the hospital admission. NLR was calculated as a ratio of absolute counts of peripheral blood neutrophils to
lymphocytes. Length of hospitalization was assessed among survivors to avoid false shortage of hospitalization time in case of early in-hospital death. Continuous data was presented as the
mean with SD or median with interquartile range (IQR), depending on the distribution of data. In comparing multiple groups, one-way ANOVA with pairwise comparisons using t tests with pooled
SD or Kruskal–Wallis rank sum test with pairwise comparisons using Mann–Whitney U test was used according to tests assumptions. Bonferroni method was used for P value adjustment. Receiver
operating characteristics (ROC) with area under the ROC curve (AUROC) analyses were preformed to measure the accuracy of absolute eosinophil count and NLR in prediction of in-hospital
mortality and to identify its cut-off values for further analysis. Variables were compared using the unpaired Student’s t-test, Welch t-test or the Wilcoxon rank sum test with continuity
correction, depending on data normality and homogeneity of variance. Categorical data were presented as absolute value and percentage. Such data were compared using Chi-square test or
Fisher’s exact test according to test assumptions. Correlation analysis was performed using Kendall's rank correlation tau. Statistical analysis was performed using R software11.
RESULTS GENERAL CHARACTERISTICS We included 275 patients. Five patients (1.82%) died in hospital. Baseline population data are presented in Table 1. Majority of patients suffered from
infectious AECOPD (n = 146; 53.09%). This group did not differ significantly in eosinophil count from non-infectious AECOPD [0.07 (0.02–0.18) vs 0.1 (0.03–0.21); _P_ = 0.09]. However, in
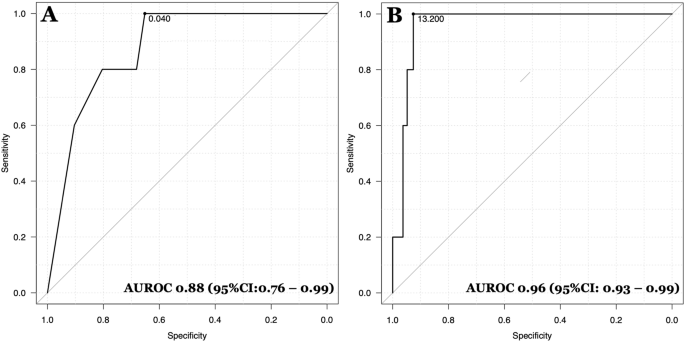
infectious AECOPD we observed significantly higher NLR values [4.3 (1.89–9.27) vs 2.6 (1–4.93); _P_ = 0.0003]. The ROC curves for absolute counts of eosinophils and NLR in peripheral blood
in prediction of in-hospital death are presented in Fig. 1. The AUROC for eosinophils was 0.88 (95% CI 0.76–0.99) and for NLR was 0.96 (95% CI 0.93–0.99). We also analyzed AUROC for the
components of NLR, however its values were lower—0.92 for lymphocyte count, identifying 1 × 103/μl as a cut-off value and 0.77 for neutrophil count with cut off value of 7.3 × 103/μl.
EOSINOPENIA In ROC analysis, an absolute number of eosinophils ≤ 0.04 × 103/µl was identified as an optimal cut-off point for eosinopenia. Using this cut-off value, eosinopenia was diagnosed
in 99 (36%) patients. All five patients who died presented on hospital admission with eosinopenia (_P_ = 0.006 for the Fisher's Exact Test). This value was characterized by sensitivity
of 100% (95% CI 35.9–100%), however specificity of 65.2% (95% CI 59.2–70.9%). The diagnostic accuracy was 0.66 (95% CI 0.6–0.71). Comparison of study parameters upon stratification by
presence of EP is presented in Table 2. We found a significant negative correlation between eosinophil count and length of hospitalization (τ = − 0.11; _P_ = 0.008), CRP (τ = − 0.11; _P_ =
0.02); WBC (τ = − 0.15; _P_ = 0.0004) and BE (τ = − 0.1; _P_ = 0.03). NLR Elevated NLR was identified when the value was ≥ 13.2. Such values were observed among 25 (9.09%) patients,
including all five patients who died during hospitalization. This cut-off point was characterized by sensitivity of 100% (95% CI 35.9–100%) and specificity estimated for 92.6% (95% CI
88.8–95.4%). The diagnostic accuracy was 0.93 (95% CI 0.9–0.96). Comparison of study parameters upon stratification by NLR value is presented in Table 3. Kendall's test did not detect
significant correlation between SaO2 and NLR (τ = − 0.06; _P_ = 0.13). In Table 2 we can see that patients who presented with eosinopenia had significantly higher NLR values: 8.44
(4.37–12.72) vs 2.26 (0.14–3.69); _P_ < 0.0001. We observed parallel situation when we analyzed results from Table 3 – patients with high NLR values had significantly lower eosinophil
count: 0.01 (0–0.02) × 103/μl vs 0.1 (0.03–0.21) × 103/μl; _P_ < 0.0001. Kendall's rank correlation tau revealed significant correlation between eosinophil and lymphocyte count: τ =
0.28 (_P_ < 0.0001) and negative correlation with NLR: τ = − 0.38 (_P_ < 0.0001). COEXISTENCE OF EOSINOPENIA WITH LYMPHOCYTOPENIA The coexistence of eosinopenia with lymphocytopenia
(defined as lymphocyte count ≤ 1 × 103/μl) was observed in 47 (17.09%) patients and only such pattern was associated with in-hospital deaths in the analyzed group. There were no deaths in
patients who presented with eosinopenia without lymphocytopenia (_P_ = 0.0001 for the Fisher's Exact Test). The coexistence of eosinopenia with lymphocytopenia was characterized by
higher specificity than previously analyzed eosinopenia [84.4% (95% CI 79.6–88.6%) vs 65.2% (95% CI 59.2–70.9%) and the same sensitivity of 100% (95% CI 35.9–100%). The diagnostic accuracy
was 0.84 (95% CI 0.8–0.89). Taking into account above findings, we reanalyzed the eosinopenia group in the context of previously analyzed study parameters. Results of additional analyses are
presented in Table 4, which illustrates study parameters upon stratification by coexistence of eosinopenia and lymphocytopenia. Kruskal Wallis rank sum test, after pairwise comparisons,
showed that only coexistence of eosinopenia with lymphocytopenia was associated with longer hospitalization (_P_ = 0.006 vs normal eosinophils and lymphocytes; _P_ = 0.02 for eosinopenia
alone, and _P_ = 0.00004 vs lymphocytopenia alone). Length of hospitalization in isolated eosinopenia or lymphocytopenia subgroups was not significantly different than in patients with
normal counts of these cells (_P_ = 1.0 and _P_ = 0.12 respectively)—Fig. 2. When we first assess the presence of coexistence of eosinopenia and lymphocytopenia, and then apply NLR, we can
achieve the best sensitivity and specificity compared to the situation when these parameters are used individually: 100% (95% CI 35.9–100) and 93.7% (95% CI 90.1–96.3), respectively. The
diagnostic accuracy for such approach was 0.94 (95% CI 0.90–0.96). Also, among survivors, occurrence of such pattern was associated with significantly longer hospital stay: 11 (7–14) vs 7
(5–10) days, P = 0.01. DISCUSSION Our aim was to assess the role of eosinopenia, lymphocytopenia and NLR as markers of in-hospital mortality and length of hospitalization (LoH) among
patients with AECOPD requiring hospitalization. Such approach seems to be justified by pathophysiological background. Namely, we would analyze eosinopenia in the context of considering
AECOPD as a state of an acute stress. Undoubtedly, COPD is associated with both physical and emotional stress. Extremal, but pictorial evidence for possible levels of stress which can be
released in this condition may be presented in context of relatively frequent association between COPD and Tako-Tsubo cardiomyopathy, which is linked with a rapid elevation of circulating
catecholamine, triggered by emotional and/or physical stress, as a key mechanism12. Also, Zurfluh et al. reported a time-dependent effect with higher levels pointing towards higher mortality
at short term associated with activation of stress hormones (particularly cortisol and cortisone)13. We should also remember that acute stress, and associated role of adrenal
glucocorticoids in this process, is not the only cause of eosinopenia in peripheral blood. There are other contributing mechanisms including migration of eosinophils to the site of
inflammation, rapid peripheral sequestration, suppression of egress of mature eosinophils from the bone marrow, and suppression of eosinophils production14,15. Eosinopenia in AECOPD was
concluded to have some clinical implications in already published studies. Namely, Holland et al.6 reported that patients with eosinopenia had a longer hospital stay and were more likely to
die in hospital. Additionally, Rahimi-Rad et al. found an association between eosinopenia and an unfavorable prognosis within 30-day after discharge7. Both Holland et al. and Rahimi-Rad et
al. used cut-off value of 40 cells/mm3 to diagnose eosinopenia. In the past, we also reported that eosinopenia would be a prognostic factor of in-hospital mortality in ECOPD16, however, in
the present study, we used the analysis which was not applied by above mentioned authors, therefore ROC curve assessment. From one hand, AUROC analysis may still justify such statement, but
from the other hand, relatively low specificity 65.2% of this marker decreased our enthusiasm significantly. Also, for further evaluation of the clinical implications of eosinopenia,
discussion of its eventual consequences should be taken into account. First, we should start with the physiological role of these cells in the immune response. Among others, eosinophils
promote humoral immunity by priming of B cells and have a role in the maintenance of type-2 immunity17, and regulation of T-helper-1 and Th2 immunity18. However, paradoxical to their
physiological effects, evidence suggests that a reduction of eosinophils appears to have no negative effect on normal health. This statement is based not only on animal studies, but also on
humans who received monoclonal antibodies reducing eosinophil count19. Therefore, even if we conclude that we indirectly assessed the exacerbation of stress or other contributing mechanisms,
the occurrence of eosinopenia itself probably has no further significant clinical importance. Taking into account all above mentioned, and the fact that glucocorticoids can reduce
eosinophils, raise neutrophils and reduce lymphocytes20,21 we decided to evaluate eosinopenia in a broader context, by adding the assessment of lymphocytopenia and NLR into analysis. The
relation between NLR and in-hospital mortality also was previously reported in patients with AECOPD22. Yao et al. presented ROC curve analysis for using NLR to predict in-hospital
mortality—AUROC was 0.803, and an optimal cut-off value was 6.24. Authors reported the sensitivity of 81.08%, and specificity of 69.17%. We observed both better sensitivity and specificity
for NLR, however we obtained higher cut-off value in ROC curve analysis. In our study, NLR presented much better accuracy parameters and higher value of AUROC than obtained for eosinopenia.
Moreover, we have observed that these parameters are not fully independent and that there is a significant relationship between the values of eosinophil count and NLR. That is why we started
to analyze these associations in the context of individual components of NLR, observing intriguing interplay between eosinophils and lymphocytes. Interestingly, patients who presented with
the coexistence of eosinopenia and lymphocytopenia had the lowest counts of both eosinophils and lymphocytes. This is justified because these patients probably had the highest level of
stress, which can suppress both types of cells. However, this relationship itself seems to also have interesting clinical implications. In turn, eosinophils and neutrophils are granulocytes
that originate from the same myeloblast progenitor in the bone marrow, and upon differentiating, each of these granulocytes leaves the marrow and migrates to the inflamed tissues to enact
their effector functions. From the other hand, lymphocytes, which originate from the different progenitor, secrete cytokines that coordinate eosinophil and neutrophil responses. From one
hand, type 2 CD4+ T cells and type 2 innate lymphoid cells produce IL-5 that prompts eosinophil production23,24, while from the other hand, Th17 cells, CD8+ T cells, γδ T cells, and type 3
innate lymphoid cells secrete IL-17A, leading to neutrophil maturation25,26. Infection by different types of pathogens may lead to different effects—either eosinophil, or neutrophil
accumulation27. Wiesner et al. reported that Rag2/IL-2Rγ−/− mice that lack lymphocytes, and observed that without lymphocytes, infected mice had significantly impaired eosinophilia compared
with similarly infected wild-type mice, yet neutrophil accumulation remained unimpaired. Authors also concluded that singular elimination of Th cells (while leaving all other lymphocyte
subsets intact, including ILCs and NK cells) may result in a loss of eosinophils that can be replaced by IL-17A-dependent neutrophilia27. Focusing on COPD population, Freeman et al. observed
decreased concentration of CD4+ and CD8+ T cells in peripheral blood during AECOPD. From the other hand, Ross et al. observed that exacerbated airway neutrophilia in cigarette smoke–exposed
mice infected with nontypeable _Haemophilus influenzae_, large subgroup of bacterial AECOPD, was associated with an induction of IL-17A28. There is also evidence for a decrease in both
total CD4+ and CD8+ T cell counts after infusion of cortisol. The effect started 90 min after infusion29. How would these issues contribute to an increase in mortality? Namely, CD4+ T cells
are major players involved in responses to infectious diseases, enabling B cells to differentiate into plasma cells, helping CD8+ T cells develop into cytotoxic cells, as well as are
required for long-term CD8 memory generation. CD4+ T cells also mediate activation of macrophages, playing a critical role in the viral and bacterial control30,31,32,33,34,35. Therefore,
decrease in this population of cells would result in catastrophic effects for homeostasis of the immune response. The above-mentioned evidence may partially and indirectly justify our
observations and allow to draw a hypothetical pathway that lymphocytopenia would be a primary pathology, which leads to eosinopenia and neutrophilia. Playing together with stress response,
which potentially aggravates such pattern, these factors may contribute to a significantly increased risk of in-hospital death. However, for confirmation of these hypotheses, there is a need
for a prospective study which directly will analyze all above mentioned relationships: stress response, lymphocytes subpopulations assessment, eosinophil and neutrophil counts with broad
profile of cytokines, including IL-17A. There are some major limitations of our study, which need to be considered. As a retrospective study, it is burdened by all limitations associated
with this type of data collection, including an absence of data regarding potential confounding factors. As the most important we indicate above mentioned lack of measurement of stress
hormones and inflammatory cytokines. It should be also worth to diagnose pathogens responsible for infectious AECOPDs. Taking into account the above-mentioned issues, the results of our
study should be considered as hypothesis generating and should be furtherly confirmed in a sufficiently powered prospective analysis, designed taking into account above mentioned
limitations. CONCLUSIONS All analyzed parameters in our study have certain value as prognostic factors of in-hospital mortality in AECOPD. However, the best profile of sensitivity and
specificity can be obtained by combined analysis of coexistence of eosinopenia and lymphocytopenia with elevated NLR. Occurrence of such pattern is also associated with significantly longer
time of hospitalization among survivors. REFERENCES * Wedzicha, J. A. & Seemungal, T. A. R. COPD exacerbations: Defining their cause and prevention. _Lancet Lond. Engl._ 370, 786–796
(2007). Article Google Scholar * Seemungal, T. A. _et al._ Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. _Am. J. Respir. Crit. Care
Med._ 157, 1418–1422 (1998). Article CAS Google Scholar * Global Initiative for Chronic Obstructive Pulmonary Disease. Global Strategy for the diagnosis, management, and prevention of
Chronic Obstructive Pulmonary Disease. https://goldcopd.org/wp-content/uploads/2019/12/GOLD-2020-FINAL-ver1.2-03Dec19_WMV.pdf. Accessed 31 October 2020. * Lima, F. V., Yen, T. Y. M. &
Patel, J. K. Trends in in-hospital outcomes among adults hospitalized with exacerbation of chronic obstructive pulmonary disease. _COPD_ 12, 636–642 (2015). PubMed Google Scholar *
Karakonstantis, S., Kalemaki, D., Tzagkarakis, E. & Lydakis, C. Pitfalls in studies of eosinopenia and neutrophil-to-lymphocyte count ratio. _Infect. Dis. Lond. Engl._ 50, 163–174
(2018). Article Google Scholar * Holland, M., Alkhalil, M., Chandromouli, S., Janjua, A. & Babores, M. Eosinopenia as a marker of mortality and length of stay in patients admitted with
exacerbations of chronic obstructive pulmonary disease. _Respirol. Carlton Vic._ 15, 165–167 (2010). Article Google Scholar * Rahimi-Rad, M. H., Asgari, B., Hosseinzadeh, N. & Eishi,
A. Eosinopenia as a marker of outcome in acute exacerbations of chronic obstructive pulmonary disease. _Maedica_ 10, 10–13 (2015). PubMed PubMed Central Google Scholar * Bolayir, A. _et
al._ The effect of eosinopenia on mortality in patients with intracerebral hemorrhage. _J. Stroke Cerebrovasc. Dis. Off. J. Natl. Stroke Assoc._ 26, 2248–2255 (2017). Article Google Scholar
* Korkmaz, Ö. _et al._ Is preoperative eosinopenia an independent predictor of early mortality for coronary artery bypass surgery?. _Heart Surg. Forum_ 19, E088-093 (2016). Article Google
Scholar * Yip, B. & Ho, K. M. Eosinopenia as a predictor of unexpected re-admission and mortality after intensive care unit discharge. _Anaesth. Intensive Care_ 41, 231–241 (2013).
Article CAS Google Scholar * R Core Team. (2018). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria.
https://www.R-project.org/. * Manfredini, R. _et al._ Heart and lung, a dangerous liaison-Tako-tsubo cardiomyopathy and respiratory diseases: A systematic review. _World J. Cardiol._ 6,
338–344 (2014). Article Google Scholar * Zurfluh, S. _et al._ Association of adrenal hormone metabolites and mortality over a 6-year follow-up in COPD patients with acute exacerbation.
_Clin. Chem. Lab. Med._ 56, 669–680 (2018). Article CAS Google Scholar * Abidi, K. _et al._ Eosinopenia is a reliable marker of sepsis on admission to medical intensive care units. _Crit.
Care Lond. Engl._ 12, R59 (2008). Article Google Scholar * Abidi, K. _et al._ Eosinopenia, an early marker of increased mortality in critically ill medical patients. _Intensive Care Med._
37, 1136–1142 (2011). Article Google Scholar * Bialas, A. _et al._ Eosinopenia as a prognostic factor in patients with acute exacerbation of chronic obstructive pulmonary disease. _Eur.
Respir. J._ 50, PA2110 (2017). Google Scholar * Spencer, L. A. & Weller, P. F. Eosinophils and Th2 immunity: Contemporary insights. _Immunol. Cell Biol._ 88, 250–256 (2010). Article
Google Scholar * Stehle, C., Saikali, P. & Romagnani, C. Putting the brakes on ILC2 cells. _Nat. Immunol._ 17, 43–44 (2016). Article CAS Google Scholar * Gleich, G. J., Klion, A. D.,
Lee, J. J. & Weller, P. F. The consequences of not having eosinophils. _Allergy_ 68, 829–835 (2013). Article CAS Google Scholar * Shoenfeld, Y., Gurewich, Y., Gallant, L. A. &
Pinkhas, J. Prednisone-induced leukocytosis. Influence of dosage, method and duration of administration on the degree of leukocytosis. _Am. J. Med._ 71, 773–778 (1981). Article CAS Google
Scholar * Altman, L. C., Hill, J. S., Hairfield, W. M. & Mullarkey, M. F. Effects of corticosteroids on eosinophil chemotaxis and adherence. _J. Clin. Invest._ 67, 28–36 (1981). Article
CAS Google Scholar * Yao, C., Liu, X. & Tang, Z. Prognostic role of neutrophil-lymphocyte ratio and platelet-lymphocyte ratio for hospital mortality in patients with AECOPD. _Int. J.
Chron. Obstruct. Pulmon. Dis._ 12, 2285–2290 (2017). Article Google Scholar * Licona-Limón, P., Kim, L. K., Palm, N. W. & Flavell, R. A. TH2, allergy and group 2 innate lymphoid
cells. _Nat. Immunol._ 14, 536–542 (2013). Article Google Scholar * Nussbaum, J. C. _et al._ Type 2 innate lymphoid cells control eosinophil homeostasis. _Nature_ 502, 245–248 (2013).
Article ADS CAS Google Scholar * Eyerich, S., Eyerich, K., Cavani, A. & Schmidt-Weber, C. IL-17 and IL-22: Siblings, not twins. _Trends Immunol._ 31, 354–361 (2010). Article CAS
Google Scholar * Zheng, Y. _et al._ Interleukin-22, a T(H)17 cytokine, mediates IL-23-induced dermal inflammation and acanthosis. _Nature_ 445, 648–651 (2007). Article CAS Google Scholar
* Wiesner, D. L., Smith, K. D., Kashem, S. W., Bohjanen, P. R. & Nielsen, K. Different lymphocyte populations direct dichotomous eosinophil or neutrophil responses to pulmonary
cryptococcus infection. _J. Immunol. Baltim. Md_ 1950(198), 1627–1637 (2017). Google Scholar * Roos, A. B. _et al._ IL-17A and the promotion of neutrophilia in acute exacerbation of chronic
obstructive pulmonary disease. _Am. J. Respir. Crit. Care Med._ 192, 428–437 (2015). Article CAS Google Scholar * Dimitrov, S. _et al._ Cortisol and epinephrine control opposing
circadian rhythms in T cell subsets. _Blood_ 113, 5134–5143 (2009). Article CAS Google Scholar * North, R. J. & Jung, Y.-J. Immunity to tuberculosis. _Annu. Rev. Immunol._ 22, 599–623
(2004). Article CAS Google Scholar * Román, E. _et al._ CD4 effector T cell subsets in the response to influenza: Heterogeneity, migration, and function. _J. Exp. Med._ 196, 957–968
(2002). Article Google Scholar * Brown, D. M., Román, E. & Swain, S. L. CD4 T cell responses to influenza infection. _Semin. Immunol._ 16, 171–177 (2004). Article CAS Google Scholar
* Sun, J. C., Williams, M. A. & Bevan, M. J. CD4+ T cells are required for the maintenance, not programming, of memory CD8+ T cells after acute infection. _Nat. Immunol._ 5, 927–933
(2004). Article CAS Google Scholar * Shedlock, D. J. & Shen, H. Requirement for CD4 T cell help in generating functional CD8 T cell memory. _Science_ 300, 337–339 (2003). Article ADS
CAS Google Scholar * Schoenberger, S. P., Toes, R. E., van der Voort, E. I., Offringa, R. & Melief, C. J. T-cell help for cytotoxic T lymphocytes is mediated by CD40-CD40L
interactions. _Nature_ 393, 480–483 (1998). Article ADS CAS Google Scholar Download references FUNDING The costs of this study were defrayed from regular finances of the Department of
Pneumology and Allergy of Medical University of Lodz, Poland (503/1-151-03). AUTHOR INFORMATION AUTHORS AND AFFILIATIONS * Department of Pneumology and Allergy, Medical University of Lodz,
Lodz, Poland Tomasz Karauda, Joanna Miłkowska-Dymanowska, Wojciech J. Piotrowski, Sebastian Majewski & Paweł Górski * Department of General and Oncological Pulmonology, Medical
University of Lodz, Lodz, Poland Kamil Kornicki & Adam Antczak * Department of Pathobiology of Respiratory Diseases, Medical University of Lodz, 22nd Kopcińskiego Street, 90-153, Lodz,
Poland Amer Jarri & Adam Jerzy Białas Authors * Tomasz Karauda View author publications You can also search for this author inPubMed Google Scholar * Kamil Kornicki View author
publications You can also search for this author inPubMed Google Scholar * Amer Jarri View author publications You can also search for this author inPubMed Google Scholar * Adam Antczak View
author publications You can also search for this author inPubMed Google Scholar * Joanna Miłkowska-Dymanowska View author publications You can also search for this author inPubMed Google
Scholar * Wojciech J. Piotrowski View author publications You can also search for this author inPubMed Google Scholar * Sebastian Majewski View author publications You can also search for
this author inPubMed Google Scholar * Paweł Górski View author publications You can also search for this author inPubMed Google Scholar * Adam Jerzy Białas View author publications You can
also search for this author inPubMed Google Scholar CONTRIBUTIONS A.J.B. conceived the idea of the study. T.K. and A.J.B. contributed to the design of the research. All authors were involved
in data collection, however with a predominance of T.K.. All authors were involved in data analysis. A.J.B. and T.K. performed statistical analysis. All authors were involved in analysis of
the results. All authors edited and approved the final version of the manuscript. CORRESPONDING AUTHOR Correspondence to Adam Jerzy Białas. ETHICS DECLARATIONS COMPETING INTERESTS The
authors declare no competing interests. ADDITIONAL INFORMATION PUBLISHER'S NOTE Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional
affiliations. RIGHTS AND PERMISSIONS OPEN ACCESS This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution
and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if
changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the
material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will
need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. Reprints and permissions ABOUT THIS ARTICLE
CITE THIS ARTICLE Karauda, T., Kornicki, K., Jarri, A. _et al._ Eosinopenia and neutrophil-to-lymphocyte count ratio as prognostic factors in exacerbation of COPD. _Sci Rep_ 11, 4804 (2021).
https://doi.org/10.1038/s41598-021-84439-8 Download citation * Received: 22 June 2020 * Accepted: 16 February 2021 * Published: 26 February 2021 * DOI:
https://doi.org/10.1038/s41598-021-84439-8 SHARE THIS ARTICLE Anyone you share the following link with will be able to read this content: Get shareable link Sorry, a shareable link is not
currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative