Clinicopathological and prognostic significance of egfr, vegf, and her2 expression in cholangiocarcinoma
- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
ABSTRACT Epidermal growth factor receptor (EGFR), vascular endothelial growth factor (VEGF), and human epidermal growth factor receptor 2 (HER2) have been considered as potential therapeutic
targets in cholangiocarcinoma, but no studies have yet clarified the clinicopathological or prognostic significance of these molecules. Immunohistochemical expression of these molecules was
assessed retrospectively in 236 cases of cholangiocarcinoma, as well as associations between the expression of these molecules and clinicopathological factors or clinical outcome. The
proportions of positive cases for EGFR, VEGF, and HER2 overexpression were 27.4, 53.8, and 0.9% in intrahepatic cholangiocarcinoma (IHCC), and 19.2, 59.2, and 8.5% in extrahepatic
cholangiocarcinoma (EHCC), respectively. Clinicopathologically, EGFR overexpression was associated with macroscopic type (_P_=0.0120), lymph node metastasis (_P_=0.0006), tumour stage
(_P_=0.0424), lymphatic vessel invasion (_P_=0.0371), and perineural invasion (_P_=0.0459) in EHCC, and VEGF overexpression with intrahepatic metastasis (_P_=0.0224) in IHCC. Multivariate
analysis showed that EGFR expression was a significant prognostic factor (hazard ratio (HR), 2.67; 95% confidence interval (CI), 1.52–4.69; _P_=0.0006) and also a risk factor for tumour
recurrence (HR, 1.89; 95% CI, 1.05–3.39, _P_=0.0335) in IHCC. These results suggest that EGFR expression is associated with tumour progression and VEGF expression may be involved in
haematogenic metastasis in cholangiocarcinoma. SIMILAR CONTENT BEING VIEWED BY OTHERS ALDEHYDE DEHYDROGENASE 3B2 PROMOTES THE PROLIFERATION AND INVASION OF CHOLANGIOCARCINOMA BY INCREASING
INTEGRIN BETA 1 EXPRESSION Article Open access 14 December 2021 CHOLANGIOCARCINOMA 2020: THE NEXT HORIZON IN MECHANISMS AND MANAGEMENT Article Open access 30 June 2020 PROGNOSTIC IMPACT OF
TUMOR MICROVESSELS IN INTRAHEPATIC CHOLANGIOCARCINOMA: ASSOCIATION WITH TUMOR-INFILTRATING LYMPHOCYTES Article 19 October 2020 MAIN Cholangiocarcinoma arises from the ductal epithelium of
the bile duct tree and is classified anatomically into intrahepatic cholangiocarcinoma (IHCC) and extrahepatic cholangiocarcinoma (EHCC). The incidence and mortality rates of
cholangiocarcinoma, especially those of IHCC, are increasing worldwide (Khan et al, 2005). Complete resection is the only way to cure the disease at present. Moreover, because
cholangiocarcinoma is difficult to diagnose at an early stage and extends diffusely, most patients have unresectable disease at clinical presentation, and prognosis is very poor (5-year
survival is 0–40% even in resected cases) (Khan et al, 2005; Sirica, 2005). Therefore, novel effective therapeutic strategies are urgently required to improve the prognosis. Among potential
therapeutic targets, several studies have revealed overexpression of epidermal growth factor receptor (EGFR) or human epidermal growth factor receptor 2 (HER2) protein, amplification, and
mutation of these genes (Ito et al, 2001; Aishima et al, 2002; Ukita et al, 2002; Altimari et al, 2003; Gwak et al, 2005; Nakazawa et al, 2005; Leone et al, 2006) as well as overexpression
of vascular endothelial growth factor (VEGF) protein (Hida et al, 1999; Tang et al, 2006) in cholangiocarcinoma. Epidermal growth factor receptor and HER2 are members of the ErbB receptor
tyrosine kinase family. Binding of ligands, such as epidermal growth factor and transforming growth factor alpha (TGF_α_), to their extracellular ligand-binding domain initiates
intracellular signalling cascades, leading to progression, proliferation, migration, and survival of cancer cells (Olayioye et al, 2000; Yarden and Sliwkowski, 2001). Vascular endothelial
growth factor plays a key role in tumour-associated neo-angiogenesis, which contributes to providing a tumour with oxygen, nutrition, and a route for metastasis. It binds to VEGFR (vascular
endothelial growth factor receptor), and leads to survival, proliferation, and migration of endothelial cell (Tabernero, 2007). Expression of these molecules has been reported to have
prognostic significance in several cancers (Gusterson et al, 1992; Han et al, 2001; Nicholson et al, 2001; Des Guetz et al, 2006; Mohammed et al, 2007). Recently, agents targeted at these
molecules have been used clinically, such as trastuzumab in breast cancer (Gonzalez Angulo et al, 2006), gefitinib, and erlotinib in non-small cell lung cancer, and bevacizumab in colorectal
cancer (Tabernero, 2007). In cholangiocarcinoma, a phase II study of erlotinib (Philip et al, 2006) and some case reports of combined chemotherapy including cetuximab (Sprinzl et al, 2006;
Huang et al, 2007) have been reported. However, no previous studies have clarified associations between the expression of these molecules and clinicopathological factors or prognosis in
patients with cholangiocarcinoma. To elucidate the biological significance and potential of these molecules as therapeutic targets, we investigated EGFR/VEGF/HER2 expression and attempted to
elucidate their associations with various clinical features as well as patient survival in 236 cases of cholangiocarcinomas. MATERIALS AND METHODS PATIENTS A total of 236 patients with
cholangiocarcinoma (male 160; female 76) who had undergone tumour resection and been diagnosed histologically as having adenocarcinoma of the bile duct at the National Cancer Center
Hospital, Tokyo, between January 1991 and August 2004, were enrolled in the present study. Median patient age and follow-up period were 65 years and 875 days, and median tumour sizes of IHCC
and EHCC were 4.8 and 3.0 cm, respectively. Detailed characteristics of patient with IHCC and EHCC are presented in Table 1, Table 2. All patients were followed for more than 100 days.
Follow-up examination was performed using computed tomography, abdominal ultrasonography, and measurement of the serum carcinoembryonic antigen and carbohydrate antigen 19–9 (CA19-9) levels
every 3–6 months. Recurrence was diagnosed by clinical, radiological, or pathological methods, but mainly by radiological evaluation including computed tomography and ultrasonography.
Clinical and pathological profiles were obtained from the database of hepatobiliary tumours based on the medical records of the patients. This study was approved by the Ethics Committee of
the National Cancer Center, Tokyo, Japan, and written informed consent was obtained from all patients. All cases were anatomically classified into two groups: IHCC and EHCC. Tumours arising
from the bilateral hepatic duct or distal common bile duct were classified as EHCC. The numbers of IHCC and EHCC cases were 106 and 130, respectively. HISTOLOGICAL ASSESSMENT Tumour staging
and histological classification were assessed according to _TNM Classification of Malignant Tumours_ (Sobin and Wittekind, 2002) defined by the International Union Against Cancer (UICC) and
the _World Health Organization Histological Classification of Tumours_ (Hamilton and Altonen, 2000). Macroscopic types of IHCC were defined with reference to _General Rules for the Clinical
and Pathological Study of Primary Liver Cancer_ (Liver Cancer Study Group of Japan, 2003): (1) the mass-forming type (MF), which develops an apparent tumour in the liver; (2) the periductal
infiltrating type (PI), which spreads along the bile duct; (3) the intraductal growth type (IG), which is confined within the bile duct, and divided into two groups: the mass-forming group
(MF and MF mixed with PI or IG) and the non-mass forming group (PI and/or IG). Macroscopic types of EHCC were divided into polypoid type and non-polypoid type (including nodular, scirrhous
constricting, and infiltrating types). Other clinicopathological factors were categorised into groups that are presented in Table 1 (IHCC) and Table 2 (EHCC). Because the classifications and
clinicopathological factors used in IHCC and EHCC are different, statistical analyses were performed separately. IMMUNOHISTOCHEMISTRY Immunohistochemistry (IHC) for EGFR, VEGF, and HER2 was
performed using a polymer-based method (Envision™+Dual Link System-HRP (Dako, DK-2600 Glostrup, Denmark)). Sources and dilutions of primary antibodies were as follows: anti-EGFR (mouse
monoclonal, clone 31G7; Zymed, South San Francisco, CA, USA; 1 : 100), anti-VEGF (rabbit polyclonal; Zymed; 1 : 50), and anti-HER2 (rabbit polyclonal; Dako; 1 : 300). Formalin-fixed,
paraffin-embedded serial tissue sections (4 _μ_m) were placed on silane-coated slides for IHC. Sections cut through the maximum tumour diameter were selected for IHC evaluation. The sections
were deparaffinised and rehydrated in xylene and grade-diluted ethanol (50–100%), and submerged for 20 min in 0.3% hydrogen peroxide with absolute methanol to block endogenous peroxidase
activity. Antigen retrieval for EGFR, VEGF, and HER2 was carried out by adding Digest-all™3 pepsin solution (Zymed) at 37°C for 10 min for EGFR, near boiling in 0.01 M citrate buffer (pH
6.0) for 15 min for VEGF, and heating in 0.01 M citrate buffer at 121°C for 10 min by pressure cooker for HER2. After protein blocking, the sections were incubated with each primary antibody
at room temperature for 1 h, followed by incubation with Envision+ Dual Link reagent at room temperature for 30 min, and visualised using 3,3′-diaminobenzidine tetrahydrochloride as a
chromogen. Finally, the sections were counterstained with haematoxylin. Sections were gently rinsed in phosphate-buffered saline between the incubation steps. EVALUATION OF
IMMUNOHISTOCHEMISTRY All sections were evaluated by DY, HO, and TS without the knowledge of any clinical or pathological information, and cases for which consensus could not be reached were
discussed to decide the evaluation. Based on the Herceptest™ (Dako) criteria, intensities of both EGFR and HER2 were defined as follows: 0, no membrane staining or membrane staining in ⩽10%
cancer cells; 1+, faint and partial membrane staining in >10% cancer cells; 2+, moderate and complete membrane staining in >10% cancer cells; 3+, strong and complete membrane staining
in >10% cancer cells. Intensities of VEGF were defined as follows: 0, no cytoplasmic staining or cytoplasmic staining in ⩽30% cancer cells; 1+, faint cytoplasmic staining, equivalent to
the intensity of normal bile duct epithelium within the same section, in >30% cancer cells; 2+, moderate cytoplasmic staining in >30% cancer cells; 3+, strong cytoplasmic staining in
>30% cancer cells. For cases showing mixed intensity, the predominant intensity was selected as the final IHC score. A final IHC score of 2+ or 3+ was defined as positive for expression
of each protein. STATISTICAL ANALYSIS Associations between results of IHC and clinicopathological factors were assessed by χ2 test. Cumulative survival rates and survival curves were
calculated by the Kaplan–Meier method, and log-rank test was performed for the comparison of survival curves. Cox's proportional hazard model was performed to estimate hazard ratio (HR)
and 95% confidence interval (CI) of each outcome (death and recurrence). Multivariate analyses were performed using the factors identified to be risk factors for each outcome by univariate
analyses, without UICC pT and UICC Stage, which are composed of other factors. All _P_-values reported are two-sided, and significance level was set at _P_<0.05. All statistical analyses
were performed with the Statview 5.0 statistical software package (Abacus Concepts, Berkeley, CA, USA). RESULTS EXPRESSION OF EGFR, VEGF, AND HER2 PROTEIN IN CHOLANGIOCARCINOMA
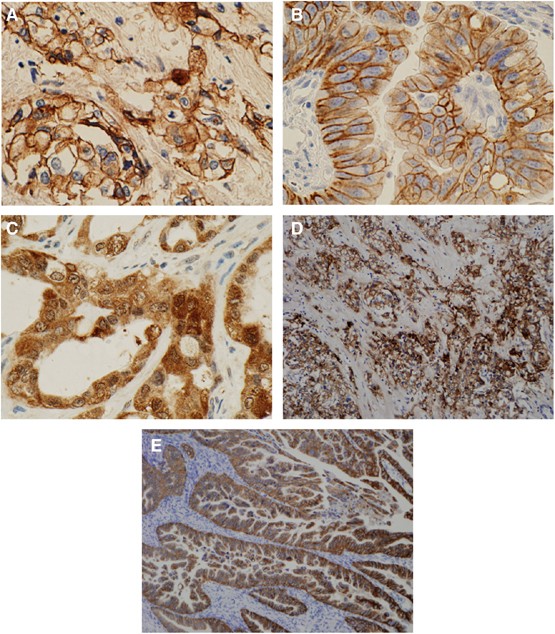
Representative cases of positive staining for each protein are shown in Figure 1 (A, EGFR; B, HER2; C, VEGF). Epidermal growth factor receptor, VEGF, and HER2 were expressed in 29 (27.4), 57
(53.8), and 1 (0.9%) of the 106 IHCCs, respectively, and in 25 (19.2), 77 (59.2), and 11 (8.5%) of the 130 EHCCs, respectively. Microscopically, EGFR was mostly overexpressed in the
moderately and/or poorly differentiated component, which is characterised by infiltration (52 of 54 EGFR-positive cases, Figure 1D), whereas only two cases showed EGFR overexpression in the
well-differentiated component. In contrast, HER2 was preferentially expressed in the well-differentiated component. In 6 of 12 HER2-positive cases, HER2 was expressed only in
well-differentiated component (Figure 1E), and 5 progressive cases showed positive HER2 staining in both the well and moderately and/or poorly differentiated components and 1 case only in
moderately differentiated component. There was no association between VEGF expression and histological features. ASSOCIATIONS BETWEEN EGFR, VEGF, AND HER2 EXPRESSION AND CLINOCOPATHOLOGICAL
FACTORS Statistical analyses of HER2 were performed only in EHCC cases because of the small number of HER2-positive cases in IHCC. In IHCC, VEGF expression was significantly associated with
intrahepatic metastasis (_P_=0.0224). There was no significant association between EGFR expression and any clinicopathological factors. In EHCC, EGFR expression was significantly associated
with macroscopic type (0% in the polypoid type, 24.0% in the non-polypoid type; _P_=0.0120), lymph node metastasis (_P_=0.0006), UICC Stage (_P_=0.0424), lymphatic vessels invasion
(_P_=0.0371), and perineural invasion (_P_=0.0459). Human epidermal growth factor receptor 2 expression was significantly associated with macroscopic type (23.8% in the polypoid type, 5.8%
in the non-polypoid type; _P_=0.0078), histological classification (25% in papillary adenocarcinoma, 9.7% in well differentiated adenocarcinoma, 3.2% in moderately differentiated
adenocarcinoma, 5.9% in poorly differentiated adenocarcinoma; _P_=0.0237), and invasion to other organs (3.9% in invasive cases, 15.1% in non-invasive cases; _P_=0.0242). VEGF expression was
not significantly associated with any factors in EHCC. Detailed results of associations between EGFR/VEGF/HER2 expression and clinicopathological factors are shown in Supplementary
information 1 (IHCC) and Supplementary information 2 (EHCC). UNIVARIATE AND MULTIVARIATE ANALYSES REGARDING OVERALL SURVIVAL AND TUMOUR RECURRENCE IN CHOLANGIOCARCINOMA The number of dead
and the median survival time were 70 cases and 724 days in IHCCs, and 76 cases and 1197 days in EHCCs, respectively. The number of recurrence and the median recurrence time were 64 cases and
522 days in IHCCs, and 78 cases and 960 days in EHCCs, respectively. Overall 5-year cumulative survival for patients with IHCC and EHCC was 33.0 and 41.6%, respectively, and no significant
difference was identified between the groups (_P_=0.0599). The survival curves stratified by EGFR expression status are shown as Figure 2. Five-year survival for patients with EGFR-positive
and EGFR-negative tumours was 17.7 and 47.1% for IHCC, and 26.4 and 45.6% for EHCC, respectively. There was a significant difference between EGFR-positive and -negative cases for both IHCC
(_P_=0.0008) and EHCC (_P_=0.0204). The results of multivariate analyses following univariate analyses regarding overall survival and tumour recurrence are shown in Table 3 (IHCC) and Table
4 (EHCC). In IHCC, 13 factors including EGFR expression were identified as significantly prognostic by univariate analysis. Multivariate analysis revealed that EGFR expression was an
independent prognostic factor (HR, 2.67; 95% CI, 1.52–4.69; _P_=0.0006), along with mass-forming macroscopic group (HR, 2.96; 95% CI, 1.06–8.31; _P_=0.0390), intrahepatic metastasis (HR,
2.91; 95% CI, 1.60–5.29; _P_=0.0005), and lymph node metastasis (HR, 1.96; 95% CI, 1.04–3.69; _P_=0.0375). In EHCC, 14 factors including EGFR expression were identified as significantly
prognostic by univariate analysis. Multivariate analysis revealed that lymph node metastasis (HR, 2.03; 95% CI, 1.16–3.55; _P_=0.0133) and a histological classification of moderately
differentiated adenocarcinoma (HR for papillary adenocarcinoma, 4.23; 95% CI, 1.08–16.50; _P_=0.0380) and poorly differentiated adenocarcinoma (HR for papillary adenocarcinoma, 13.22; 95%
CI, 3.10–56.45; _P_=0.0005) were significant prognostic factors. Multivariate analysis following univariate analysis for risk factors of tumour recurrence revealed that EGFR expression in
IHCC was a significant risk factor of tumour recurrence (HR, 1.89; 95% CI, 1.05–3.39; _P_=0.0335), along with intrahepatic metastasis (HR, 2.36; 95% CI, 1.31–4.25; _P_=0.0044), lymph node
metastasis (HR, 2.24; 95% CI, 1.19–4.22; _P_=0.0126), and venous invasion (HR, 6.74; 95% CI, 1.31–34.73; _P_=0.0225), whereas, in EHCC, lymph node metastasis (HR, 1.75; 95% CI, 1.03–2.98;
_P_=0.0394) and dissected periductal structures margin (HR, 1.81; 95% CI, 1.03–3.16; _P_=0.0383) were independent risk factors of tumour recurrence, but EGFR expression was not associated
with tumour recurrence even in univariate analysis. DISCUSSION This study, analysing EGFR/VEGF/HER2 expression in the largest cohort of cholangiocarcinoma reported so far, showed for the
first time that EGFR expression in IHCC is significantly associated with poor prognosis. In addition, our study confirmed previously reported prognostic factors in cholangiocarcinoma, such
as macroscopic type, intrahepatic metastasis, lymph node metastasis, and histological classification (Yamamoto et al, 1998; Ohtsuka et al, 2002; Morimoto et al, 2003; DeOliveira et al,
2007). Expression of EGFR or HER2 is known to be a prognostic factor in some cancers (Gusterson et al, 1992; Nicholson et al, 2001), but no previous study has clarified the influence of
these molecules on prognosis in cholangiocarcinoma (Ito et al, 2001; Altimari et al, 2003; Nakazawa et al, 2005), probably because cholangiocarcinoma is a relatively rare cancer and
collection of a large cohort is difficult. Indeed, most previous studies were performed on the basis of only 50 cases at most. Although it is unclear why EGFR expression in IHCC is an
independent prognostic factor, it may be associated with frequent relapse of cancer because EGFR expression is also a risk factor for tumour recurrence. In contrast to IHCC, EGFR expression
was not an independent prognostic factor in EHCC, but was associated with clinical features that may represent tumour progression and invasion, such as lymph node metastasis and apparent
stromal invasion in EHCC. Because cancer tissue tends to be heterogeneous, histological diagnosis is generally decided on the basis of the degree of differentiation that predominates. In
order to elucidate the biological significance of each protein, we microscopically examined positive cases in detail and compared their expression with histological components, and found
that EGFR tended to be expressed in the poorly differentiated component, which is characterised by infiltration in both IHCC and EHCC. Similar results have been reported in bladder cancer
(Neal et al, 1985), oesophageal adenocarcinoma (Wilkinson et al, 2004), and IHCC (Ito et al, 2001), although the studies were based on small cohorts. These findings indicate that EGFR
expression may be a relatively late event in the development of cholangiocarcinoma and associated with invasion and progression. Because it has been previously reported that poor
differentiation is associated with unfavourable outcome in other cancers (Sohn et al, 2000; Hassan et al, 2005), the association between EGFR expression and poor differentiation may also be
a reason that EGFR expression is a prognostic factor. Though the prognostic factors were different between IHCC and EHCC, it may be due to the difference of anatomical character, which
extrahepatic bile duct is near from other organs and is not surrounded by liver parenchyma in contrast to intrahepatic bile duct. The intrahepatic epithelium is distinct from the
extrahepatic epithelium in terms of development and differentiation (Shiojiri, 1997), and the risk factors, pathogenesis, and clinical features of IHCC and EHCC are different (Strom et al,
1985; Nakeeb et al, 1996; Shaib et al, 2007). Although no previous studies have elucidated EGFR function in normal bile duct epithelium, EGFR overexpression might play distinct roles in IHCC
and EHCC. Vascular endothelial growth factor expression was detected frequently, being evident in about 60% of our study cases, which is consistent with previous studies (31.4–75.6%) (Hida
et al, 1999; Tang et al, 2006). Our study revealed that VEGF expression was significantly associated with intrahepatic metastasis in IHCC. Vascular endothelial growth factor is a key
molecule in angiogenic pathway. Angiogenesis is an essential component in the process of metastasis, and this has been partly confirmed by studies showing that microvessel density (MVD) is
associated with metastasis and a poorer outcome in a range of cancers (Weidner et al, 1991; Zetter, 1998). It has also been reported that high MVD is an independent prognostic factor in
node-negative IHCC (Shirabe et al, 2004) and is associated with VEGF expression in IHCC (Tang et al, 2006), although no study has clarified the involvement of angiogenesis in the process of
metastasis in cholangiocarcinoma. Our result suggests that VEGF plays an important role in the process of cholangiocarcinoma metastasis by promoting angiogenesis. Human epidermal growth
factor receptor 2 was expressed in only 11 of 130 EHCC cases (8.5%) and in one of 106 IHCC cases (0.9%). The proportion of HER2-positive cases reported previously has varied from 4.2 to
81.8% (Ito et al, 2001; Aishima et al, 2002; Ukita et al, 2002; Altimari et al, 2003; Nakazawa et al, 2005), and the discrepancy may be due to differences in staining procedure or tumour
location. In contrast to EGFR expression, HER2 expression was associated with more favourable clinical features, such as a polypoid macroscopic type and absence of other organ involvement.
The proportion of HER2-positive cases in papillary adenocarcinoma was higher than in other histological types, consistent with some previous reports claiming that HER2 expression in
cholangiocarcinoma is associated with an early disease stage (Endo et al, 2002; Nakazawa et al, 2005). Microscopically, HER2 is preferentially expressed in well differentiated component, and
it is also expressed in dedifferentiated components (moderately and/or poorly differentiated components) in progressive cases. This indicates that HER2 overexpression is maintained from an
early stage of carcinogenesis in cases that are HER2-positive. Recently, the efficacy of molecular targeting therapy for various molecules including EGFR/VEGF/HER2 has been proved clinically
in a wide range of cancers. Epidermal growth factor receptor inhibitor has been reported to be effective in a cholangiocarcinoma cell line (Yoon et al, 2004), and a phase II study of
erlotinib, an EGFR inhibitor, in patients with advanced biliary cancer has been reported. In this study, the progression-free rate at 6 months as a primary end point was 17% (7/42) despite
the fact that disease condition was severe, and the disease control rate was 50% (20/42) (Philip et al, 2006). This study suggested the clinical applicability of the EGFR inhibitor to
cholangiocarcinoma. Several clinical trials demonstrating the efficacy of VEGF inhibition for other cancers have been reported (Hurwitz et al, 2004; Sandler et al, 2006), and VEGF
upregulation in tumour cells is considered to be a mechanism of resistance to EGFR inhibitors (Viloria Petit et al, 2001). Therefore, dual inhibition of both EGFR and VEGF may exert a
synergistic effect. In summary, we have shown that EGFR and VEGF expression is relatively common in cholangiocarcinoma. Moreover, in IHCC, EGFR expression is an independent prognostic factor
and VEGF expression is associated with intrahepatic metastasis. In EHCC, EGFR expression is associated with clinical factors involved in tumour progression and invasion. Our results suggest
the validity and significance of molecular targeting agents for EGFR and/or VEGF pathway, and that further preclinical and clinical studies are warranted for improving the clinical outcome
of cholangiocarcinoma. CHANGE HISTORY * _ 16 NOVEMBER 2011 This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication _
REFERENCES * Aishima SI, Taguchi KI, Sugimachi K, Shimada M, Sugimachi K, Tsuneyoshi M (2002) c-erbB-2 and c-Met expression relates to cholangiocarcinogenesis and progression of intrahepatic
cholangiocarcinoma. _Histopathology_ 40 (3): 269–278 Article Google Scholar * Altimari A, Fiorentino M, Gabusi E, Gruppioni E, Corti B, D'Errico A, Grigioni WF (2003) Investigation
of ErbB1 and ErbB2 expression for therapeutic targeting in primary liver tumours. _Dig Liver Dis_ 35 (5): 332–338 Article CAS Google Scholar * DeOliveira ML, Cunningham SC, Cameron JL,
Kamangar F, Winter JM, Lillemoe KD, Choti MA, Yeo CJ, Schulick RD (2007) Cholangiocarcinoma: thirty-one-year experience with 564 patients at a single institution. _Ann Surg_ 245 (5): 755–762
Article Google Scholar * Des Guetz G, Uzzan B, Nicolas P, Cucherat M, Morere JF, Benamouzig R, Breau JL, Perret GY (2006) Microvessel density and VEGF expression are prognostic factors in
colorectal cancer. Meta-analysis of the literature. _Br J Cancer_ 94 (12): 1823–1832 Article CAS Google Scholar * Endo K, Yoon BI, Pairojkul C, Demetris AJ, Sirica AE (2002) ERBB-2
overexpression and cyclooxygenase-2 up-regulation in human cholangiocarcinoma and risk conditions. _Hepatology_ 36 (2): 439–450 Article CAS Google Scholar * Gonzalez Angulo AM, Hortobagyi
GN, Esteva FJ (2006) Adjuvant therapy with trastuzumab for HER-2/neu-positive breast cancer. _Oncologist_ 11 (8): 857–867 Article CAS Google Scholar * Gusterson BA, Gelber RD, Goldhirsch
A, Price KN, Säve-Söderborgh J, Anbazhagan R, Styles J, Rudenstam CM, Golouh R, Reed R, Martinez-Tello F, Tiltman A, Torhorst J, Grigolato P, Bettelheim R, Neville AM, Bürki K, Castiglione
M, Collins J, Lindtner J, Senn HJ (1992) Prognostic importance of c-erbB-2 expression in breast cancer. International (Ludwig) breast cancer study group. _J Clin Oncol_ 10 (7): 1049–1056
Article CAS Google Scholar * Gwak GY, Yoon JH, Shin CM, Ahn YJ, Chung JK, Kim YA, Kim TY, Lee HS (2005) Detection of response-predicting mutations in the kinase domain of the epidermal
growth factor receptor gene in cholangiocarcinomas. _J Cancer Res Clin Oncol_ 131: 649–652 Article CAS Google Scholar * Hamilton SR, Altonen LA (2000) _World Health Organization
Classification of Tumours: pathology & Genetics: Tumours of the Digestive System_. Lyon: IARCPress Google Scholar * Han H, Silverman JF, Santucci TS, Macherey RS, d'Amato TA, Tung
MY, Weyant RJ, Landreneau RJ (2001) Vascular endothelial growth factor expression in stage I non-small cell lung cancer correlates with neoangiogenesis and a poor prognosis. _Ann Surg Oncol_
8 (1): 72–79 Article CAS Google Scholar * Hassan C, Zullo A, Risio M, Rossini FP, Morini S (2005) Histologic risk factors and clinical outcome in colorectal malignant polyp: a
pooled-data analysis. _Dis Colon Rectum_ 48 (8): 1588–1596 Article Google Scholar * Hida Y, Morita T, Fujita M, Miyasaka Y, Horita S, Fujioka Y, Nagashima K, Katoh H (1999) Vascular
endothelial growth factor expression is an independent negative predictor in extrahepatic biliary tract carcinomas. _Anticancer Res_ 19 (3B): 2257–2260 CAS PubMed Google Scholar * Huang
TW, Wang CH, Hsieh CB (2007) Effects of the anti-epidermal growth factor receptor antibody cetuximab on cholangiocarcinoma of the liver. _Onkologie_ 30 (3): 129–131 CAS PubMed Google
Scholar * Hurwitz H, Fehrenbacher L, Novotny W, Cartwright T, Hainsworth J, Heim W, Berlin J, Baron A, Griffing S, Holmgren E, Ferrara N, Fyfe G, Rogers B, Ross R, Kabbinavar F (2004)
Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. _N Engl J Med_ 350 (23): 2335–2342 Article CAS Google Scholar * Ito Y, Takeda T, Sasaki Y,
Sakon M, Yamada T, Ishiguro S, Imaoka S, Tsujimoto M, Higashiyama S, Monden M, Matsuura N (2001) Expression and clinical significance of the erbB family in intrahepatic cholangiocellular
carcinoma. _Pathol Res Pract_ 197 (2): 95–100 Article CAS Google Scholar * Khan SA, Thomas HC, Davidson BR, Taylor Robinson SD (2005) Cholangiocarcinoma. _Lancet_ 366 (9493): 1303–1314
Article Google Scholar * Leone F, Cavalloni G, Pignochino Y, Sarotto I, Ferraris R, Piacibello W, Venesio T, Capussotti L, Risio M, Aglietta M (2006) Somatic mutations of epidermal growth
factor receptor in bile duct and gallbladder carcinoma. _Clin Cancer Res_ 12: 1680–1685 Article CAS Google Scholar * Liver Cancer Study Group of Japan (2003) _General Rules for the
Clinical and Pathological Study of Primary Liver Cancer_, 2nd English edn. Tokyo: Kanehara & Co. LTD * Mohammed RA, Green A, El Shikh S, Paish EC, Ellis IO, Martin SG (2007) Prognostic
significance of vascular endothelial cell growth factors-A, -C and -D in breast cancer and their relationship with angio- and lymphangiogenesis. _Br J Cancer_ 96 (7): 1092–1100 Article CAS
Google Scholar * Morimoto Y, Tanaka Y, Ito T, Nakahara M, Nakaba H, Nishida T, Fujikawa M, Ito T, Yamamoto S, Kitagawa T (2003) Long-term survival and prognostic factors in the surgical
treatment for intrahepatic cholangiocarcinoma. _J Hepatobiliary Pancreat Surg_ 10 (6): 432–440 Article Google Scholar * Nakazawa K, Dobashi Y, Suzuki S, Fujii H, Takeda Y, Ooi A (2005)
Amplification and overexpression of c-erbB-2, epidermal growth factor receptor, and c-met in biliary tract cancers. _J Pathol_ 206 (3): 356–365 Article CAS Google Scholar * Nakeeb A, Pitt
HA, Sohn TA, Coleman J, Abrams RA, Piantadosi S, Hruban RH, Lillemoe KD, Yeo CJ, Cameron JL (1996) Cholangiocarcinoma. A spectrum of intrahepatic, perihilar, and distal tumors. _Ann Surg_
224 (4): 463–473 Article CAS Google Scholar * Neal DE, Marsh C, Bennett MK, Abel PD, Hall RR, Sainsbury JR, Harris AL (1985) Epidermal-growth-factor receptors in human bladder cancer:
comparison of invasive and superficial tumours. _Lancet_ 1 (8425): 366–368 Article CAS Google Scholar * Nicholson RI, Gee JM, Harper ME (2001) EGFR and cancer prognosis. _Eur J Cancer_ 37
(Suppl 4): S9–S15 Article CAS Google Scholar * Ohtsuka M, Ito H, Kimura F, Shimizu H, Togawa A, Yoshidome H, Miyazaki M (2002) Results of surgical treatment for intrahepatic
cholangiocarcinoma and clinicopathological factors influencing survival. _Br J Surg_ 89 (12): 1525–1531 Article CAS Google Scholar * Olayioye MA, Neve RM, Lane HA, Hynes NE (2000) The
ErbB signaling network: receptor heterodimerization in development and cancer. _EMBO J_ 19 (13): 3159–3167 Article CAS Google Scholar * Philip PA, Mahoney MR, Allmer C, Thomas J, Pitot
HC, Kim G, Donehower RC, Fitch T, Picus J, Erlichman C (2006) Phase II study of erlotinib in patients with advanced biliary cancer. _J Clin Oncol_ 24 (19): 3069–3074 Article CAS Google
Scholar * Sandler A, Gray R, Perry MC, Brahmer J, Schiller JH, Dowlati A, Lilenbaum R, Johnson DH (2006) Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancer. _N
Engl J Med_ 355 (24): 2542–2550 Article CAS Google Scholar * Shaib YH, El Serag HB, Nooka AK, Thomas M, Brown TD, Patt YZ, Hassan MM (2007) Risk factors for intrahepatic and extrahepatic
cholangiocarcinoma: a hospital-based case-control study. _Am J Gastroenterol_ 102 (5): 1016–1021 Article Google Scholar * Shiojiri N (1997) Development and differentiation of bile ducts in
the mammalian liver. _Microsc Res Tech_ 39 (4): 328–335 Article CAS Google Scholar * Shirabe K, Shimada M, Tsujita E, Aishima S, Maehara S, Tanaka S, Takenaka K, Maehara Y (2004)
Prognostic factors in node-negative intrahepatic cholangiocarcinoma with special reference to angiogenesis. _Am J Surg_ 187 (4): 538–542 Article Google Scholar * Sirica AE (2005)
Cholangiocarcinoma: molecular targeting strategies for chemoprevention and therapy. _Hepatology_ 41: 5–15 Article Google Scholar * Sobin LH, Wittekind CH (2002) _TNM Classification of
Malignant Tumours_, 6th edn. New York: Wiley-Liss Inc Google Scholar * Sohn TA, Yeo CJ, Cameron JL, Koniaris L, Kaushal S, Abrams RA, Sauter PK, Coleman J, Hruban RH, Lillemoe KD (2000)
Resected adenocarcinoma of the pancreas-616 patients: results, outcomes, and prognostic indicators. _J Gastrointest Surg_ 4 (6): 567–579 Article CAS Google Scholar * Sprinzl MF,
Schimanski CC, Moehler M, Schadmand Fischer S, Galle PR, Kanzler S (2006) Gemcitabine in combination with EGF-Receptor antibody (Cetuximab) as a treatment of cholangiocarcinoma: a case
report. _BMC Cancer_ 6: 190 Article Google Scholar * Strom BL, Hibberd PL, Soper KA, Stolley PD, Nelson WL (1985) International variations in epidemiology of cancers of the extrahepatic
biliary tract. _Cancer Res_ 45 (10): 5165–5168 CAS PubMed Google Scholar * Tabernero J (2007) The role of VEGF and EGFR inhibition: implications for combining anti-VEGF and anti-EGFR
agents. _Mol Cancer Res_ 5 (3): 203–220 Article CAS Google Scholar * Tang D, Nagano H, Yamamoto H, Wada H, Nakamura M, Kondo M, Ota H, Yoshioka S, Kato H, Damdinsuren B, Marubashi S,
Miyamoto A, Takeda Y, Umeshita K, Dono K, Wakasa K, Monden M (2006) Angiogenesis in cholangiocellular carcinoma: expression of vascular endothelial growth factor, angiopoietin-1/2,
thrombospondin-1 and clinicopathological significance. _Oncol Rep_ 15 (3): 525–532 CAS PubMed Google Scholar * Ukita Y, Kato M, Terada T (2002) Gene amplification and mRNA and protein
overexpression of c-erbB-2 (HER-2/neu) in human intrahepatic cholangiocarcinoma as detected by fluorescence _in situ_ hybridization, _in situ_ hybridization, and immunohistochemistry. _J
Hepatol_ 36: 780–785 Article CAS Google Scholar * Viloria Petit A, Crombet T, Jothy S, Hicklin D, Bohlen P, Schlaeppi JM, Rak J, Kerbel RS (2001) Acquired resistance to the antitumor
effect of epidermal growth factor receptor-blocking antibodies _in vivo_: a role for altered tumor angiogenesis. _Cancer Res_ 61 (13): 5090–5101 CAS PubMed Google Scholar * Weidner N,
Semple JP, Welch WR, Folkman J (1991) Tumor angiogenesis and metastasis – correlation in invasive breast carcinoma. _N Engl J Med_ 324 (1): 1–8 Article CAS Google Scholar * Wilkinson NW,
Black JD, Roukhadze E, Driscoll D, Smiley S, Hoshi H, Geradts J, Javle M, Brattain M (2004) Epidermal growth factor receptor expression correlates with histologic grade in resected
esophageal adenocarcinoma. _J Gastrointest Surg_ 8 (4): 448–453 Article Google Scholar * Yamamoto M, Takasaki K, Yoshikawa T, Ueno K, Nakano M (1998) Does gross appearance indicate
prognosis in intrahepatic cholangiocarcinoma? _J Surg Oncol_ 69 (3): 162–167 Article CAS Google Scholar * Yarden Y, Sliwkowski MX (2001) Untangling the ErbB signalling network. _Nat Rev
Mol Cell Biol_ 2 (2): 127–137 Article CAS Google Scholar * Yoon JH, Gwak GY, Lee HS, Bronk SF, Werneburg NW, Gores GJ (2004) Enhanced epidermal growth factor receptor activation in human
cholangiocarcinoma cells. _J Hepatol_ 41 (5): 808–814 Article CAS Google Scholar * Zetter BR (1998) Angiogenesis and tumor metastasis. _Annu Rev Med_ 49: 407–424 Article CAS Google
Scholar Download references ACKNOWLEDGEMENTS This work was supported in part by Foundation for Promotion of Cancer Research (FPCR), Japan, grant-in-aid for the Comprehensive
10-Year-Strategy for Cancer Control from the Ministry of Health, Labor and Welfare, Japan and the Program for Promotion of Fundamental Studies in Health Sciences of the National Institute of
Biomedical Innovation (NiBio), Japan. DY is a recipient of a Research Resident Fellowship from FPCR. AUTHOR INFORMATION AUTHORS AND AFFILIATIONS * Cancer Genomics Project, National Cancer
Center Research Institute, Tokyo, Japan D Yoshikawa & T Shibata * Division of Gastroenterological and General Surgery, Department of Surgery, Asahikawa Medical College, Asahikawa, Japan
D Yoshikawa & S Kasai * Pathology Division, National Cancer Center Research Institute, Tokyo, Japan H Ojima, N Hiraoka, S Hirohashi & T Shibata * Epidemiology and Prevention
Division, Research Center for Cancer Prevention and Screening, National Cancer Center, Tokyo, Japan M Iwasaki * Hepato-Biliary and Pancreatic Surgery Division, National Cancer Center
Hospital, Tokyo, Japan T Kosuge Authors * D Yoshikawa View author publications You can also search for this author inPubMed Google Scholar * H Ojima View author publications You can also
search for this author inPubMed Google Scholar * M Iwasaki View author publications You can also search for this author inPubMed Google Scholar * N Hiraoka View author publications You can
also search for this author inPubMed Google Scholar * T Kosuge View author publications You can also search for this author inPubMed Google Scholar * S Kasai View author publications You can
also search for this author inPubMed Google Scholar * S Hirohashi View author publications You can also search for this author inPubMed Google Scholar * T Shibata View author publications
You can also search for this author inPubMed Google Scholar CORRESPONDING AUTHOR Correspondence to T Shibata. ADDITIONAL INFORMATION Supplementary Information accompanies the paper on
British Journal of Cancer website (http://www.nature.com/bjc) SUPPLEMENTARY INFORMATION SUPPLEMENTARY INFORMATION 1 (DOC 33 KB) RIGHTS AND PERMISSIONS From twelve months after its original
publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit
http://creativecommons.org/licenses/by-nc-sa/3.0/ Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Yoshikawa, D., Ojima, H., Iwasaki, M. _et al._ Clinicopathological and
prognostic significance of EGFR, VEGF, and HER2 expression in cholangiocarcinoma. _Br J Cancer_ 98, 418–425 (2008). https://doi.org/10.1038/sj.bjc.6604129 Download citation * Received: 30
August 2007 * Revised: 13 November 2007 * Accepted: 15 November 2007 * Published: 18 December 2007 * Issue Date: 29 January 2008 * DOI: https://doi.org/10.1038/sj.bjc.6604129 SHARE THIS
ARTICLE Anyone you share the following link with will be able to read this content: Get shareable link Sorry, a shareable link is not currently available for this article. Copy to clipboard
Provided by the Springer Nature SharedIt content-sharing initiative KEYWORDS * cholangiocarcinoma * epidermal growth factor receptor * vascular endothelial growth factor * human epidermal
growth factor receptor 2 * immunohistochemistry * prognosis